juvenile Form des Morbus Alexander

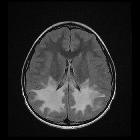
Atypical MRI
features in familial adult onset Alexander disease: case report. Axial Brain MRI showed low T1-weighted signals (a), high T2-weighted signals (b), and hyperintensity in FLAIR image(c) around the periventricular area. MRI with contrast enhancement was normal (d). DWI revealed slight hyperintensity (e). MRA were normal (f)

Atypical MRI
features in familial adult onset Alexander disease: case report. Axial spinal MRI showed hyperintensity involving the corticospinal tracts extends from the carotid 2 (a arrowhead) to carotid 7 cord (b arrowhead) in T2WI image, mild atrophy of cervical spinal cord in sagittal T1WI image (c), severe atrophy of whole thoracic segments in sagittal T2WI image, which is similar to the typical “tadpole” (d), medullary atrophy at 3 years after onset (e, f), and severe medulla and cerebellar atrophy 1 years later (g, h)

A case report
of adult-onset Alexander disease clinically presenting as Parkinson’s disease: is the comorbidity associated with genetic susceptibility?. Brain MRI and FP-CIT PET imaging of the patient. a, b Brain MRI with T2-weighted axial images show typical bilateral high signal intensity at both medulla oblongata and cerebellar dentate nuclei. c No major lesions in the basal ganglia and periventricular white matter. d A T1-weighted sagittal image shows tadpole shape cervicomedullary atrophy. e 3-dimensional [18F] FP-CIT PET shows severely decreased dopaminergic uptake in bilateral putamen and caudate nucleus with a rostrocaudal gradient. f FP-CIT PET in control shows normal dopaminergic uptake in bilateral putamen and caudate nucleus


 Assoziationen und Differentialdiagnosen zu juvenile Form des Morbus Alexander:
Assoziationen und Differentialdiagnosen zu juvenile Form des Morbus Alexander: