Kawasaki-Syndrom

















Kawasaki disease (KD) is a small to medium vessel vasculitis predominantly affecting young children. It can affect any organ but there is a predilection for the coronary vessels.
Epidemiology
Japan has the highest incidence in the world, with an annual incidence of 300/100,000 children under the age of four years . Worldwide, it is the commonest vasculitis in children . It is slightly more common in males, M: F, 1.4:1 .
It is more common in siblings, ~3% of siblings will be diagnosed with Kawasaki, this equates to a ten-fold increased risk in a sibling. It is also more likely in children of affected parents, although no genetic link has been identified .
In the United States, it is most commonly seen in children of Asian ethnicity, in particular, Japanese, but less commonly in African Americans and least commonly in Caucasians.
Since April 2020, rare cases of a Kawasaki-like disorder have been reported in critically-ill children who are COVID-19 positive. A true causative association between SARS-CoV-2, the cause of COVID-19, and Kawasaki disease has not been established as yet .
Clinical presentation
Persistent fever is the commonest way with which most children present. The specific signs and symptoms vary with the stage of the disease:
Acute stage
- fever that is refractory to antibiotics
- general malaise and irritability
- non-exudative conjunctivitis (90%)
- anterior uveitis (70%)
- perianal erythema (70%)
- lymphadenitis (75%)
- strawberry tongue
Subacute stage
- desquamation of the digits
- thrombocytosis
- coronary artery aneurysms
- highest risk of death
Convalescent stage
- clinical symptoms and signs recede
Chronic stage
- persistence of any cardiac complications into adulthood
Pathology
An autoimmune etiology has been postulated. It is generally self-limiting but acute fatalities are thought to occur in ~1% of cases. The most concerning morbidity is due to coronary involvement where it can manifest as myocarditis with coronary arterial aneurysm formation .
Radiographic features
Plain radiograph
Chest radiographs can be normal. Abnormal findings are non-specific and include a reticulogranular pattern, peribronchial cuffing, pleural effusion, atelectasis and/or air trapping .
Rarely, a few years after resolution of the initial episode, the patient may present with calcified coronary artery aneurysms visible on the chest x-ray . Although rare, this is an Aunt Minnie presentation of Kawasaki disease sequelae in older patients.
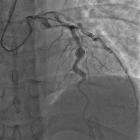
Coronary angiography / CT angiography
May show small coronary arterial ectasias, aneurysms or stenoses. Angiography is the most sensitive and specific for vascular assessment .
Coronary artery aneurysms can be classified as :
- small: <5 mm
- medium: 5–8 mm
- large: >8 mm
Coronary stenosis is more common in the left coronary artery while intracoronary thrombus is more frequently observed in the right coronary artery .
MRI / MR angiography
Useful in assessing myocardial perfusion, wall thinning and aneurysms.
Echocardiography
Transthoracic echocardiography especially useful in the approach to patients who fall short of full clinical criteria (incomplete KD), as the presence of the following is diagnostic :
- coronary artery dilation
- dilation which exceeds the mean coronary artery diameters by 2.5 standard deviations is classified as aneurysmal
- left ventricular dysfunction
- mitral regurgitation
- manifestation of endocardial inflammation
- pericardial effusion
History and etymology
It is named after the Japanese pediatrician Tomisaku Kawasaki (1925-2020) who saw his first case in 1961 and initially described it in a case series of 50 children in 1967 .
Siehe auch:
- Aneurysma
- Vaskulitis
- Aneurysma Koronararterien
- Kawasaki-Syndrom mit Gallenblasenbeteiligung
- Aunt Minnie
- Fibromuskuläre Dysplasie der Koronarien
und weiter:


 Assoziationen und Differentialdiagnosen zu Kawasaki-Syndrom:
Assoziationen und Differentialdiagnosen zu Kawasaki-Syndrom:
