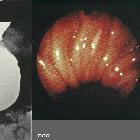
Mallory-Weiss tear
Mallory-Weiss tears occur due to violent projection of gastric contents against the lower esophagus, which results in mucosal and submucosal tear with involvement of the venous plexus. The resultant clinical syndrome is known as Mallory-Weiss syndrome.
Clinical presentation
Patients present with painless hematemesis.
Pathology
Tears most commonly involve the distal esophagus at the gastro-esophageal junction. It is more common in alcoholics or after episodes of binge drinking, after repeated episodes of retching or vomiting.
Radiographic features
Fluoroscopy
On a contrast swallow study, there may be a leak of contrast.
CT
A mucosal laceration without transmural perforation is likely to be occult on CT. However, CT images of the esophagus many occasionally show evidence of hemorrhage or foci of extraluminal gas at a site of mucosal injury .
Treatment and prognosis
Unless there is persistent bleeding, the treatment like that of other mucosal lacerations, is supportive . Most patients with upper gastrointestinal hemorrhage from a Mallory-Weiss tear cease bleeding spontaneously and do not require specific therapy .
History and etymology
It was first described in 1929 by George Kenneth Mallory (1900-1986), American pathologist, and Soma Weiss (1898-1942), American physician .
Differential diagnosis
- Boerhaave syndrome: no hematemesis as there is complete transmural disruption of the esophageal wall with blood escaping into the mediastinum
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Mallory-Weiss-Syndrom:
Assoziationen und Differentialdiagnosen zu Mallory-Weiss-Syndrom: