Meckel-Divertikel










































Meckel diverticulum is a congenital intestinal diverticulum due to fibrous degeneration of the umbilical end of the omphalomesenteric (vitelline) duct that occurs around the distal ileum. It is considered the most common structural congenital anomaly of the gastrointestinal tract.
Epidemiology
Approximately 2% (range 0.3-3%) of all individuals may have a Meckel diverticulum (see the rule of 2s). While traditionally described to have increased male predilection, it may occur with equal frequency in both sexes although symptoms from complications are more common in male patients . Most patients with a complication are thought to present in the first two years of life .
Clinical presentation
A large proportion of individuals remain asymptomatic although up to a third of them may experience clinical symptoms. The incidence of complications with a Meckel diverticulum is reported to wide range between 4% and 40% of patients; however, one retrospective study showed the lifetime risk of developing complications of the Meckel diverticulum is 4% up to the age of 20 years, 2% up to the age of 40 years, and zero in the elderly population . There is an increased incidence of the Meckel diverticulum in Crohn patients compared to the general population:
- gastrointestinal hemorrhage (melena/hematochezia): most common complication and may account for ~30% of symptomatic cases . Large mostly self-limiting bright red rectal bleed.
- small-bowel obstruction: second most common presentation
- adhesion or mesodiverticular band
- luminal obstruction from diverticulitis or foreign body impacted in the diverticulum or enterolith formation
- volvulus
- intussusception: particularly if the diverticulum inverts
- internal hernia from a persistent attachment of the diverticulum to the umbilicus by the obliterated omphalomesenteric duct
- Littre hernia: inclusion of the diverticulum into a hernia
- neoplastic obstruction
- inclusion of a Meckel diverticulum in a true knot that forms between the ileum and sigmoid.
- inflammation (diverticulitis): Meckel diverticulitis
- perforation
- neoplasm arising in a Meckel diverticulum
Pathology
Gross anatomy
Meckel diverticulum is a true diverticulum (i.e. all layers of the gastrointestinal tract are present in its wall) and arises from the antimesenteric border of the small intestine.
It can be as long as 5 cm with diameters up to 2 cm. Most (75%) Meckel diverticula are found within 60 cm (range 40-100 cm) of the ileocecal valve . It can be seen in the midline, or on either side of the midline. However, midline and right iliac fossa location are the commonest. Its level on CT can be either superior or inferior to the terminal ileum .
Blood supply
- arterial supply typically arises from the omphalomesenteric artery (arising from an ileal branch of the superior mesenteric artery)
Histology
Meckel diverticula are lined with heterotopic mucosa in up to 60% of cases:
- gastric mucosa ~62%
- pancreatic ~6%
- gastric and pancreatic ~5%
- jejunal ~2%
- Brunner glands ~2%
- gastric and duodenal ~2%
Development
It is considered a remnant of the omphalomesenteric-vitelline duct, which connects the yolk sac to the midgut through the umbilical cord. This duct is typically obliterated by the 5-8 week of gestation. Failure of closure results in:
- diverticulum (~90% of cases)
- omphalomesenteric fistula
- enterocyst
- fibrous band
Radiographic features
Imaging these may occasionally be detected incidentally or may be identified if there is a complication.
Fluoroscopy
Small bowel enemas have sometimes been used for the diagnosis in some centers, although a precise technique is required if the diagnosis is to be excluded with any degree of certainty .
Ultrasound
Usually of limited use in the diagnosis of an uncomplicated Meckel diverticulum. Ultrasound may show a blind-ending peristaltic loop connected to the small bowel.
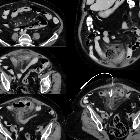
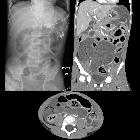
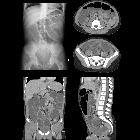
CT
CT is of limited value in uncomplicated cases, as the diverticulum may resemble a normal bowel loop. CT may show a fluid- or air-filled blind-ending pouch that arises from the antimesenteric side of the distal ileum.
It is possible for the diverticulum to invert and appear as an intraluminal polypoid lesion .
Angiography or CT angiography
When investigated in the context of gastrointestinal hemorrhage, angiography/CT angiography may show the persistent omphalomesenteric artery in most individuals with a Meckel diverticulum although recognition of the artery may be difficult due to overlying vessels.
Scintigraphy
Scintigraphy with Tc-Na-pertechnetate has a limited sensitivity (~60%) ; however, it aids in the diagnosis of diverticula with ectopic gastric mucosa. Pertechnetate is taken up by mucin-secreting cells of the gastric mucosa and ectopic gastric tissue. Higher sensitivity may be present in children (~85-90%).
History and etymology
It is named after the German anatomist Johann Friedrich Meckel (the younger), (1781-1833) who described its anatomy and embryology in 1809 .
Siehe auch:
- Appendicitis epiploica
- Divertikulitis
- Appendizitis
- Dünndarmdivertikulitis
- omphalomesenteric duct cyst
- Meckeldivertikulitis
- Ductus omphaloentericus
und weiter:
- Dünndarmileus
- Bauchwandhernien
- Meckel-Syndrom
- Normvarianten der Pankreasgänge
- Urachuszyste
- Heterotopie des Pankreas
- Dünndarmdivertikel
- untere gastrointestinale Blutung
- dysencephalia spanchnocystica
- Littre´sche Hernie
- ektope Magenschleimhaut
- patent omphalomesenteric duct of a Meckel's diverticulum
- carcinoid tumour in Meckel's diverticulum
- ektope Magenschleimhaut in Meckeldivertikel
- Meckel-Divertikel Perforation
- ileokolische Invagination durch Meckel-Divertikel
- Fremdkörper in Meckel-Divertikel
- Divertikel des Gastrointestinaltraktes
- Dünndarmvolvulus durch Meckel-Divertikel
- Divertikel
- meckel diverticulum with gastric mucosa


 Assoziationen und Differentialdiagnosen zu Meckel-Divertikel:
Assoziationen und Differentialdiagnosen zu Meckel-Divertikel: