Mundbodenphlegmone
Ludwig angina (cellulitis) refers to rapidly progressive inflammation of the floor of mouth, which is potentially life-threatening due to the risk of rapid airway compromise.
Epidemiology
Largely due to the advent of antibiotics, the condition is uncommon in present day modern societies. Immunocompromised patients are at higher risk.
Clinical presentation
Usually, the patient has signs and symptoms of preceding dental infection. Due to the anatomy of the submandibular, sublingual and submental spaces and the mylohyoid muscle, spread of infection can occur between these spaces. Subsequent swelling can displace the tongue superiorly and posteriorly leading to potential airway obstruction and asphyxiation. When severe, the floor of mouth swelling can also cause trismus, odynophagia and dysphagia. The classic signs are a brawny, tender non-fluctuant induration of the submandibular space, with an elevation of the tongue.
Three characteristics of Ludwig angina can be remembered as the 3 Fs: feared, often fatal but rarely fluctuant .
When left untreated, this infection can spread inferiorly into the neck and mediastinum.
Pathology
Ludwig angina is a rapidly-spreading life-threatening cellulitis of the floor of mouth, involving the submandibular, sublingual, and submental spaces.
Most cases (85%) are thought to originate from an untreated odontogenic infection (most commonly the second and third mandibular molars ), mainly Streptococcus spp., Staphylococcus spp., and Bacteroides spp. . Of the other 15% of cases, causes include :
- peritonsillar or parapharyngeal abscess
- sialadenitis
- epiglottitis
- penetrating injuries to the floor of the mouth
Radiographic features
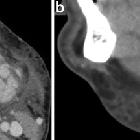
It is primarily a clinical diagnosis. Imaging may be performed to assess for airway patency and the presence of an underlying dental abscess. Generally, there is diffuse edema within and between the affected submandibular, sublingual, or submental spaces. The presence of an abscess involving any of these spaces may raise concern. Accompanying swelling and elevation of the tongue may also be present.
Treatment and prognosis
The most important aspect of treatment is the protection of the airway for which tracheostomy may be required. Aggressive intravenous antibiotics are the mainstay of therapy and intravenous steroids may help reduce the swelling and hence risk of airway compromise. Drainable collections are treated urgently with surgical decompression.
History and etymology
It is named after Wilhelm Frederick von Ludwig (1790-1865) , a German physician who first described this condition in 1836 . Notably, he died in December 1865 from 'non-specific neck inflammation' which some believe was Ludwig angina .
Angina in this context is being used in its more general sense of an intense localized pain, rather than the specific pain of cardiac ischemia.
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Mundbodenphlegmone:
Assoziationen und Differentialdiagnosen zu Mundbodenphlegmone:




