peritonsillar abscess











Peritonsillar abscess or quinsy is the most common deep neck infection, almost always secondary to acute or recurrent tonsillitis.
Epidemiology
Peritonsillar abscesses are most common in 20-40 year-olds with a predominance for males and for smokers. It is less common in children but immunosuppression increases the risk of development .
Clinical presentation
Clinical features include a unilateral odynophagia, dysphagia, voice changes (sometimes classically referred to as a ‘hot potato’ voice), trismus, and excessive drooling . Additionally, patients may be systemically unwell with fever and malaise .
Pathology
Peritonsillar abscess is usually a complication of tonsillitis and thus has a similar clinical presentation and infective etiology . The most common pathogens are those that cause tonsillitis, namely beta-hemolytic Streptococci, with Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae also common causes .
Infection extends through the fibrous capsule of the tonsil entering the peritonsillar space, located between the tonsillar capsule and superior pharyngeal constrictor muscle. Further extension may occur into the parapharyngeal, masticator, and/or submandibular spaces.
Radiographic features
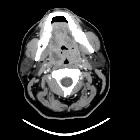
CT
- rim-enhancing fluid collection adjacent to an enlarged and inflamed tonsil
- 75% specific and 100% sensitive at diagnosing peritonsillar abscess
- false positives are due to the similar appearances of peritonsillar abscess and phlegmon
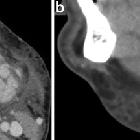
Ultrasound
Point-of-care ultrasonography has been utilized for the diagnosis of peritonsillar abscess, as well as for procedural guidance for incision and drainage when indicated. Intraoral use of an endocavitary transducer is most common; when limited by trismus or patient discomfort, submandibular scanning is possible with a curvilinear or linear probe. Findings include :
- complex, hypoechoic collection 5-25 mm anteromedial to the internal carotid artery
- internal carotid/jugular vein may be identified with color flow Doppler
- probe pressure may elicit movement of the debris within the abscess
- heterogeneous, poorly defined margins
- may also demonstrate surrounding hyperechoic rim
- color flow or power Doppler may demonstrate circumferential hyperemia
Treatment and prognosis
Peritonsillar abscesses almost always require surgical aspiration or incision and drainage in comparison to tonsillitis, which is normally managed with antibiotics.
Complications
- retropharyngeal effusion
- retropharyngeal abscess
- septic thrombophlebitis of the internal jugular vein (Lemierre syndrome)
Differential diagnosis
- tonsillitis with phlegmon
- intratonsillar abscess
- retropharyngeal abscess
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Peritonsillarabszess:
Assoziationen und Differentialdiagnosen zu Peritonsillarabszess: