nabothian cyst
Nabothian cysts, also known as a retention cysts of the cervix , are non-neoplastic cystic lesions that occur in relation to the uterine cervix.
Terminology
Nabothian is generally written without capitalization, i.e. 'nabothian', and not 'Nabothian', as it is an adjectival form derived from a name, not the name itself.
Epidemiology
They are common and some reports suggest that they may be seen in up to 12% of routine pelvic MRI scans .
Clinical presentation
The majority are asymptomatic, although in rare cases they can enlarge and become symptomatic or present with vaginal discharge.
Pathology
They represent retention cysts of the cervix that occur as a result of chronic inflammation and healing. They are thought to form as a result of the healing process of chronic cervicitis and represent mucinous cysts due to obstruction from an overgrowth of squamous epithelium.
Symptomatic nabothian cysts can also occur as a late complication of subtotal hysterectomy, in which internalisation of the transformation zone and partial obliteration of the canal are postulated as predisposing factors.
Size
Nabothian cysts are usually small spanning a few millimeters in diameter but on occasion, have been reported reach extreme sizes of up to 4 cm.
Variants
Tunnel cluster: a special type of nabothian cyst, is characterized by complex multicystic dilatation of the endocervical glands.
Radiographic features
Ultrasound
Typically seen an anechoic well defined cystic lesions near the endocervical canal. If the cysts are large, the cervical region can appear enlarged . Color Doppler interrogation shows no associated color flow.
CT
If small may not be detectable on CT. May occasionally be seen as a focal low attenuation region within the cervical region.
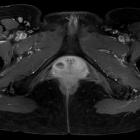
MRI
They may be seen as well-circumscribed single or multiple cystic lesions within the cervical stroma.
Signal characteristics typically follow that of fluid .
- T1
- iso- to hypointense relative to muscle in typical cases
- very rare cases with mucin may show some high signal
- T2: cysts are hyperintense relative to muscle
- T1 C+ (Gd): there is no associated enhancement and typically have no solid enhancing components
Treatment and prognosis
Most nabothian cysts are clinically insignificant. The majority of cases are not treated because the cysts are entirely benign; however, an excision biopsy is sometimes indicated in large, complex, cystic lesions to rule out rare forms of mucus-producing neoplasia, including adenoma malignum .
History and etymology
Nabothian cysts were first described by Guillaume Desnoues (1650–1735), a French surgeon in 1681, who thought that they represented a store of spermatic-related substances. The German physician, Martin Naboth (1675–1721) published a monograph on female sterility in 1707 and felt that the cysts were a collection of the woman's ova .
Differential diagnosis
General imaging differential considerations include:
- cystic cervicitis
- adenoma malignum: minimal deviation adenocarcinoma (MDA) of the cervix
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Ovula Nabothi:
Assoziationen und Differentialdiagnosen zu Ovula Nabothi: