Nebenmilz









 nicht verwechseln mit: Splenose
nicht verwechseln mit: SplenoseSplenunculi, also known as supernumerary spleens, accessory spleens, or splenules, are small nodules of spleen that are separate from the rest of the organ.
Epidemiology
They are common, seen in up to 16% of CTs of the abdomen and up to 30% of autopsies .
Pathology
Accessory spleens are congenital nodules of normal splenic tissue. The spleen forms from multiple smaller components during embryogenesis and failure of this fusion can lead to one or more nodules remaining separate . Each component is extraperitoneal. They should not be confused with splenosis (see below) which is acquired and intraperitoneal.
Clinical presentation
They are benign and asymptomatic, so their importance is mainly related to the need to distinguish them from more sinister pathology.
In patients who undergo splenectomy for autoimmune disorders (most commonly idiopathic thrombocytopenic purpura and autoimmune hemolytic anemia), the growth of unrecognized accessory spleens is a classic cause of late relapse. Thus, accessory spleens should be identified preoperatively to ensure their removal.
Radiographic features
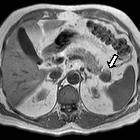
Splenunculi are typically a few centimeters in diameter when identified, well-circumscribed rounded or ovoid nodules. Although most are located near the spleen, they have been identified elsewhere in the abdominal cavity including :
- splenic hilum (most common)
- gastrosplenic ligament
- splenorenal ligament
- pancreatic tail
- greater omentum
- small bowel mesentery
- stomach or bowel wall
- scrotum
CT
They have density and enhancing characteristics similar to the rest of the spleen. Small (<1 cm) and may appear hypodense compared with the spleen, most likely as an artefact of partial volume .
The converse of this is that if a mass is seen at the splenic hilum, which does not enhance in the same fashion as the adjacent spleen, then alternative diagnoses should be entertained.
Nuclear medicine
Tc99m sulfur colloid scan
In rare instances, the diagnosis can be confirmed with a Tc99m sulfur colloid scan which will demonstrate increased uptake as long as the splenunculus is at least 2 cm in diameter.
Tc99m heat-denatured red blood cell scan
Splenic tissue (spleen and accessory spleens) will demonstrate intense physiological uptake .
Treatment and prognosis
Accessory spleens generally do not require any form of treatment . They are resected together with the spleen when performing a total splenectomy for conditions such as blood dyscrasias and hemoglobinopathy.
Resection is also considered when infarction, torsion or ruptured accessory spleen due to vascular pedicle complications .
Differential diagnosis
General imaging differential considerations include:
- peritoneal metastases
- lymph node enlargement
- tail of pancreas tumor or metastases
- renal tumor recurrence post-nephrectomy
- adrenal mass
- pancreatic neuroendocrine tumors
Other conditions with abnormal location or morphology of splenic tissue include:
- lobulations or clefts: represent incomplete but partial fusion and are very common
- polysplenia: rarely multiple splenules are seen without a 'parent' spleen; this is referred to as polysplenia and is seen associated with situs abnormalities
- splenosis: splenic tissue deposits following abdominal trauma or surgery (e.g. splenectomy), and do not have splenic arterial supply
- wandering spleen: spleen located in an unusual position within the abdominal cavity
Siehe auch:
- Nebennierenraumforderungen
- Splenose
- Pankreastumoren
- ektopes Milzgewebe
- intrapankreatische Nebenmilz
- doppelte Milz
- Polysplenie-Syndrom
- Metastasen
- Howell-Jolly-Körperchen
- situs abnormalities
und weiter:


 Assoziationen und Differentialdiagnosen zu Nebenmilz:
Assoziationen und Differentialdiagnosen zu Nebenmilz: