ovarian cyst
















Ovarian cysts are commonly encountered in gynecological imaging, and vary widely in etiology, from physiologic, to complex benign, to neoplastic.
Pathology
Small cystic ovarian structures should be considered normal ovarian follicles unless the patient is pre-pubertal, post-menopausal, pregnant, or the mean diameter is >3 cm (see the 1-2-3 rule).
Types of cysts
- physiological cysts: mean diameter ≤3 cm
- functional cysts (can produce hormones):
- follicular cysts of the ovary (estrogen): >3 cm
- corpus luteum cysts (progesterone)
- theca lutein cyst: gestational trophoblastic disease
- complications in functional cysts:
- hemorrhagic ovarian cyst
- enlargement
- rupture
- torsion
- other cysts:
- multiple large ovarian cysts in ovarian hyperstimulation syndrome
- postmenopausal cyst: serous inclusion cysts of the ovary
- polycystic ovaries
- ovarian torsion
- ovarian cystic neoplasm
Radiographic features
Ultrasound is usually the first imaging modality for assessment of ovarian lesions.
Imaging features of simple ovarian cysts:
- anechoic
- intraovarian or exophytic
- imperceptible wall
- posterior acoustic enhancement: may not be as obvious with harmonic or compound imaging
- visible far wall
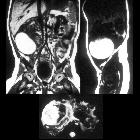
A cyst may become large enough to obscure the ovary from which it is arising.
Radiology report
The Society of Radiologists in Ultrasound made in 2019 the following recommendations regarding reporting of simple adnexal cysts of suspected ovarian origin based on size and menopausal status :
- premenopausal women
- ≤3 cm: no need to report; if described, consider calling a "follicle" rather than a "cyst" to reduce patient anxiety
- impression: normal ovaries/adnexa
- recommendation: no follow-up
- >3 to ≤5 cm: report presence of simple cyst(s) and largest cyst diameter
- impression: benign finding in the physiologic size range
- recommendation: no follow-up
- >5 cm: report with all cyst diameters
- impression: benign simple cyst
- recommendation:
- >5 to ≤7 cm: follow-up either in 2-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment, but no follow up is needed if the cyst is exceptionally well-visualized/characterized and documented with confidence by the imager
- >7 cm: follow-up either in 2-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment
- follow-up of cyst (previously >5 cm): describe in report with all cyst diameters if not resolved
- decreased in size
- impression: benign inconsequential finding; decrease in size excludes neoplasm
- recommendation: no further follow-up needed
- similar in size
- impression: benign simple cyst with stability over ≥12 months, most likely nonneoplastic or very slow growing benign neoplasm
- recommendation: follow-up at 2 years from initial study to document stability and understand growth rate
- increased in size
- impression: enlarging simple cyst, most likely a benign neoplasm
- recommendation: follow-up in 1 year to evaluate any further changes in size
- decreased in size
- ≤3 cm: no need to report; if described, consider calling a "follicle" rather than a "cyst" to reduce patient anxiety
- postmenopausal women
- ≤1 cm: no need to report
- impression: normal ovaries/adnexa
- recommendation: no follow-up
- >1 to ≤3 cm: report presence of simple cyst(s) and largest cyst diameter
- impression: benign inconsequential finding
- recommendation: no follow-up
- >3 cm: report with all cyst diameters
- impression: benign simple cyst
- recommendation:
- >3 to ≤5 cm: follow-up either in 3-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment, but no follow up is needed if the cyst is exceptionally well-visualized/characterized and documented with confidence by the imager
- >5 cm: follow-up either in 3-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment
- follow-up of cyst (previously >3 cm): describe in report with all largest cyst diameters if not resolved
- decreased in size
- impression: benign simple cyst; decrease in size excludes neoplasm
- recommendation: no further follow-up needed
- similar in size
- impression: benign simple cyst
- recommendation: follow-up at 2 years from initial study to document stability
- increased in size
- impression: enlarging simple cyst, most likely a benign neoplasm
- recommendation: follow-up in 1 year to evaluate any further changes in size
- decreased in size
- ≤1 cm: no need to report
Note that these guidelines do not apply to hemorrhagic ovarian cysts.
Treatment and prognosis
- large (>3 cm) or symptomatic cysts may undergo surgical resection
- smaller asymptomatic cysts are treated conservatively
- risk of malignancy in septated ovarian cysts with no papillary projections or solid components are also considered low and are usually followed up on ultrasound
See also
Siehe auch:
- eingeblutete Ovarialzyste
- gestational trophoblastic disease
- Ovarialtorsion
- Corpus luteum
- polycystic ovaries
- Corpus luteum Zyste
- zystische Ovarialtumoren
- follicular cysts of the ovary
- Ovarielles Hyperstimulationssyndrom
- ovarian theca lutein cysts
- Paraovarialzysten
- neonatale Ovarialzyste
- Ovarialfollikel
- torsion
und weiter:
- seröses Zystadenom des Ovars
- ovaries
- ovarian follicular cyst
- sonographic values in obstetrics and gynaecology
- Ovar
- functional ovarian cyst
- large for dates uterus
- gynäkologisch radiologisches Curriculum
- seröses Zystadenokarzinom des Ovars
- transposed ovaries
- para fimbrial cyst
- para-ovarian cyst
- para ovarian cystadenoma
- mesothelial cysts
- hyperreactio luteinalis
- functional ovarian cyst size
- hydatid cyst of Morgagni
- para tubal cyst
- seromuzinöses Zystadenom des Ovars
- torquierte Ovarialzyste
- tarlov cysts mimicing bilateral adnexial cystic masses
- pränatal torquierte, infarzierte Ovarialzyste


 Assoziationen und Differentialdiagnosen zu Ovarialzyste:
Assoziationen und Differentialdiagnosen zu Ovarialzyste: