pulmonale Lymphangiektasie



Pulmonary lymphangiectasia (PL) refers to a rare, fatal congenital abnormality of the lungs characterized by grossly dilated lymphatic channels in the sub pleural, interlobar, perivascular and peribronchial areas .
It is divided into two main types :
- cardiac-associated lymphangiectasia (secondary type)
- non-cardiac associated lymphangiectasia (primary type)
- early-onset type
- late-onset type
Clinical presentation
Clinical features depend on the type:
- cardiac-associated lymphangiectasia (secondary type)
- cyanosis and respiratory depression
- non-cardiac associated lymphangiectasia (primary type)
- early-onset type
- abnormal pattern of respiration
- late-onset type
- progressive pattern of lung disease starting at 10 days old
- early-onset type
Pathology
Abnormal development of the lungs and associated lymphatics during 14th to 20th week of gestation .
During the intrauterine life, in this phase of gestation, the lymphatics in the sub pleural space and interlobular areas are large and decrease in caliber by the 20th week. However, continued development of the lung without decrease in size of lymphatics results in this abnormality.
Associations
- cardiac-associated lymphangiectasia (secondary type)
- there is variable configuration of the heart depending on the underlying cardiac malformation; most commonly:
- TAPVR to SVC, innominate vein, ductus venosus and portal vein
- hypoplastic left heart
- TGA
- there is variable configuration of the heart depending on the underlying cardiac malformation; most commonly:
- non-cardiac associated lymphangiectasia (primary type)
- early-onset type
- congenital ichthyosis
- Ehlers-Danlos syndrome
- polycystic kidney disease
- dysplastic kidneys
- uretero-pelvic obstruction
- urethral stenosis
- left ventricular hypertrophy
- late-onset type
- obstructive uropathy
- cystic fibrosis
- early-onset type
Radiographic features
Antenatal ultrasound
- hydrops fetalis (associated feature)
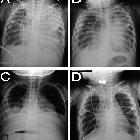
Plain radiograph
- perihilar infiltrates
- pleural effusion
- varying degrees of hyperinflation
HRCT
- perihilar infiltrates with air bronchograms
- interstitial and interlobular septal thickening
- pleural effusion (chylothorax)
MRI
- T1 (especially coronal):
- interstitial thickening
- pleural effusion
- atelectasis
- T2 (especially axial)
- usually shows high-signal material within the pulmonary interstitium
Lymphoscintigraphy
- radiotracer accumulation in the lungs
- asymmetric visualization of lymphatic channels
Treatment and prognosis
Cardiac associated and the non-cardiac associated early onset types are more fatal leading to death. The late onset type does not have a poor prognosis as symptoms and clinical findings improve after the first year of life .
See also
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu
Assoziationen und Differentialdiagnosen zu 