Splenic embolization

Review of
proximal splenic artery embolization in blunt abdominal trauma. 65 year old female undergoing celiac angiogram for upper gastrointestinal bleed. Celiac DSA showing the dorsal pancreatic artery (thin arrows) arising directly from the celiac trunk (dotted black arrow), which occurs in ~ 15% of cases. The great pancreatic artery (curved black arrow) arises from the mid portion of the splenic artery. Ideal placement of coils/plugs in proximal splenic artery embolization is between these two vessels. Transverse pancreatic artery (thick black arrow)

Review of
proximal splenic artery embolization in blunt abdominal trauma. 32 year old male in a snowmobile verses truck accident. a Celiac DSA after proximal splenic artery embolization with an AMPLATZER™ Plug (black star). Note the dorsal pancreatic artery (thin straight black arrow) originates from the common hepatic artery, a variation that occurs in approximately 20% of cases. Blood from the dorsal pancreatic artery then travels left along the transverse pancreatic artery (thick black arrows). Blood then flows retrograde up the great pancreatic artery (curved black arrow) reconstituting the mid/distal splenic artery (thick white arrow). b Subsequent image shows reconstituted flow in the mid/distal splenic artery (thick white arrow) with opacification of splenic artery branches (thin white arrows)

Review of
proximal splenic artery embolization in blunt abdominal trauma. 52 yo male status post motor vehicle accident with grade 3 splenic injury. After coils were mistakenly placed distal to the origin of the great pancreatic artery (thin white arrow a, b), splenic artery DSA shows there is reconstitution of the distal splenic artery (thin black arrows b-d) via a great pancreatic artery to transverse pancreatic artery (thick white arrow b) to caudal pancreatic artery (curved white arrow b) pathway. The caudal pancreatic artery arises from the distal third of the splenic artery (70% of cases) or an inferior polar branch of the splenic artery (30% of cases)

Review of
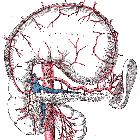
proximal splenic artery embolization in blunt abdominal trauma. Schematic for the dorsal pancreatic (thin white arrow) to transverse pancreatic (thick white arrow) to great pancreatic artery (curved white arrow). Short black arrows denote the direction of flow. (Black star-coils in proximal splenic artery)

Review of
proximal splenic artery embolization in blunt abdominal trauma. Transradial splenic angiogram following splenic trauma. After proximal splenic artery embolization using coils (black star), flow from the proximal splenic artery (straight white arrow) to the distal splenic artery (curved white arrow) is maintained via dorsal pancreatic (straight thin black arrow) to transverse pancreatic (straight thick black arrow) to great pancreatic artery (curved black arrow) pathway

Review of
proximal splenic artery embolization in blunt abdominal trauma. 85 year old male with pancreatic cancer status post iatrogenic trauma following drain placement for a perisplenic abscess. Splenic artery DSA after embolization shows that the AMPLATZER™ Plug (white arrow) has mistakenly been placed distal to the great pancreatic artery (curved black arrow). This excludes collateral perfusion of the spleen via the dorsal pancreatic artery (straight thin black arrow) to transverse pancreatic (thick black arrows) to great pancreatic artery pathway

Review of
proximal splenic artery embolization in blunt abdominal trauma. Schematic representation of collateral pathway of right gastroepiploic (thick curved black arrow) to left gastroepiploic artery (thin curved black arrow). The right gastroepiploic artery is a terminal branch of the gastrodoudenal artery (GDA; straight white arrow). It courses within the greater omentum along the greater curvature of the stomach. The left gastroepiploic artery may arise from the distal splenic or an inferior polar artery

Review of
proximal splenic artery embolization in blunt abdominal trauma. 56 year old female, history of alcoholism, fall from standing height. Celiac artery angiogram after proximal splenic artery embolization with an AMPLATZERTM Plug (star a). This shows collateral perfusion to the spleen and distal splenic artery (straight black arrows b-d) via GDA (thin straight white arrow b, c) → right gastroepiploic (curved white arrow b-d) → left gastroepiploic pathway (curved black arrow b-d). Note that the parenchymal opacification of the spleen is markedly delayed compared to the liver, an expected finding after PSAE (d). Corkscrew intrahepatic arteries and the recannalized periumbilical vein with hepatopedal flow (thick white arrow b, c) are consistent with the patient’s known history of alcohol cirrhosis and portal hypertension

Review of
proximal splenic artery embolization in blunt abdominal trauma. a Schematic of collateral splenic perfusion via the left gastric (star) to short gastric pathway (curved arrows). Note that the normal direction of flow is reversed in the short gastric arteries. b 39 year old female with history of splenic laceration caused by motor vehicle accident 11 years prior which was treated with a subtotal splenectomy as well as splenic artery and vein ligation. Left gastric artery angiogram done for bleeding gastric varices demonstrates the left gastric to short gastric to spleen collateral pathway

Review of
proximal splenic artery embolization in blunt abdominal trauma. 37 year old male with an AAST grade III splenic injury following high speed motor vehicle crash. a Splenic artery DSA with a catheter in the splenic artery (black arrow) demonstrating a focal pseudoaneurysm (white arrows). b A base catheter in the splenic artery (small white arrow), with a 5 F microcatheter fed through a tortuous splenic artery (large white arrow). The tortuosity and distance of this pseudoaneurysm precludes the use of traditional covered stents in this area. c Post coil embolization DSA showing a treated pseudoaneurysm. d One week after embolization, an axial contrast enhanced CT through the spleen demonstrates distal embolization coils (small white arrow), an area of focal infarction (small black arrow), and a splenic abscess (large black arrow). A partially visualized drain is present within the infected collection (large white arrow)

School ager
with hypersplenism. AP image from a splenic angiogram (left) shows an extremely enlarged spleen. AP image from a splenic angiogram obtained after embolization with polyvinyl alcohol 250 to 350 micron particles (right) shows the spleen to be reduced in size by 75%.The diagnosis was splenomegaly treated with partial splenectomy via embolization.

Splenic
artery embolization • Splenic laceration with embolization - Ganzer Fall bei Radiopaedia

Splenic
artery embolization • Traumatic splenic laceration (grade IV) with splenic artery pseudoaneurysm - Ganzer Fall bei Radiopaedia

Splenic
artery embolization • Post splenic artery glue embolization material (chest x-ray) - Ganzer Fall bei Radiopaedia

Medical
devices in the abdomen and pelvis • Splenic embolization coils - Ganzer Fall bei Radiopaedia

Splenic
artery embolization • Splenic infarction - Ganzer Fall bei Radiopaedia
Splenic (artery) embolization is an endovascular technique for treatment of splenic and splenic artery pathology as an alternative to splenic artery ligation or splenectomy. It often results in successfully treating the underlying pathology, while maintaining at least partial splenic function.
Indications
- traumatic splenic injury, particularly AAST grade III-V in haemodynamically stable patients
- hypersplenism
- splenic malignancy
- splenic steal syndrome
- splenic artery aneurysm or pseudoaneurysm
Technique
There are a multitude of techniques including:
- partial or complete embolization
- proximal or distal embolization
- coil, particle or glue embolization
Complications
- left pleural effusion and atelectasis (20-50%)
- splenic infarct (~3%)
- splenic abscess (~2%)
Long term immune function
In contrast to patients who undergo splenectomy, patients who undergo splenic artery embolization are demonstrated to have preserved immune function at long term follow up. This evidence is supported by research studies that report the lack of circulating Howell jolly bodies on follow up.
Siehe auch:
- Milzhämatom
- Arteria lienalis
- Arteria pancreatica magna
- Pankreasarterien
- Embolisation der Milzarterie bei Pankreaspseudozyste
- Embolisation der Milzarterie bei Pankreasverletzungen
und weiter:


 Assoziationen und Differentialdiagnosen zu Embolisation der Milzarterie:
Assoziationen und Differentialdiagnosen zu Embolisation der Milzarterie: