Tenosynovial giant cell tumor




















Tenosynovial giant cell tumors are usually benign lesions that arise from the tendon sheath. It is unclear whether these lesions represent neoplasms or merely reactive masses. On imaging, these lesions are commonly demonstrated as localized, solitary, subcutaneous soft tissue nodules, with low T1 and T2 signal and moderate enhancement.
Terminology
Tenosynovial giant cell tumor is the term used in the latest (2013) World Health Organization classification . They have previously been known as giant cell tumors of the tendon sheath (GCTTS), pigmented villonodular tumor of the tendon sheath (PVNTS), extra-articular pigmented villonodular tumor of the tendon sheath or localized or focal nodular synovitis .
Epidemiology
Typically, they present in the 3to 5 decades and have a slight female predilection with an F:M ratio of 1.5-2.1:1 . They are the second most common soft tissue mass of the hand and wrist.
Clinical presentation
Clinically these masses generally present in the hand (although they are found elsewhere also) as localized swelling with or without pain. They are slow-growing.
Pathology
Tenosynovial giant cell tumors can cause pressure erosion of adjacent bone, or rarely can invade the bone mimicking an intraosseous lesion .
Macroscopic appearance
Tenosynovial giant cell tumors have been divided macroscopically into localized or diffuse forms and appear as rubbery multinodular masses that are well circumscribed. They have an enveloping fibrous capsule, and the transected surface of the specimen is variably colored depending on the relative proportions of fibrous tissue, hemosiderin, and pigmented foam cells .
Histology
The tumor is histologically identical to pigmented villonodular synovitis (PVNS) and is composed of fibroblasts and multinucleated giant cells, foamy histiocytes, and inflammatory cells on a background fibrous matrix .
Radiographic features
Plain radiograph
As these masses arise from tendons, commonly of the hand, they may cause pressure erosions on the underlying bone in 10-20% of cases. More commonly these masses arise from the palmar tendons. The mass itself is of soft tissue density. Periosteal reaction and calcification are uncommon .
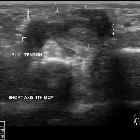
Ultrasound
Ultrasound is useful as it allows not only the characterization of the lesion but also is able to demonstrate the relationship with the adjacent tendon. On the dynamic scan, there is free movement of the tendon within the lesion. Typically they appear as:
- associated with the volar surface of the digits
- does not move with flexion or extension of adjacent tendons
- usually homogeneously hypoechoic, although some heterogeneity may be seen in echotexture in a minority of cases
- most will have some internal vascularity
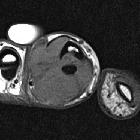
MRI
Not surprisingly, given the histological similarity to PVNS, giant cell tumors of the tendon sheaths also share the same finding on MRI, mainly on account of hemosiderin accumulation.
Signal characteristics
- T1: low signal
- T2: low signal
- T1 C+ (Gd): often show moderate enhancement
- GE: low and may demonstrate blooming
Treatment and prognosis
Tenosynovial giant cell tumors are usually benign and local surgical excision usually suffices, with local recurrence (seen in 10-20% of cases) requiring more extensive surgery with or without radiotherapy being uncommon . Locally aggressive and malignant tenosynovial giant cell tumors can occur . Metastases can occur, most commonly to lymph nodes and lung .
Differential diagnosis
General imaging differential considerations include:
- ganglion cyst
- cystic component
- attached to underlying joint capsule or tendon sheath
- if previously ruptured may appear similar
- pigmented villonodular synovitis (PVNS)
- histologically identical
- involves larger joints
- desmoid tumor
- fibroma of the tendon sheath
- overlapping imaging features
- no susceptibility artifact on gradient echo sequences
- histologically diagnosis often needed
- fibrosarcoma
- rheumatoid arthritis nodules
If in the hand consider:
- glomangioma: has high T2 signal on MRI
Siehe auch:
- synoviale Osteochondromatose
- Gelenkerguss
- Pigmentierte villonoduläre Synovialitis
- Riesenzelltumor
- Lipoma arborescens
- Ganglion (Überbein)
- siderotic synovitis
- glomangioma
- Desmoid-Tumor - aggressive Fibromatose
- Lokalisation Riesenzelltumor der Sehnenscheide
und weiter:
- Riesenzelltumor des Knochens
- WHO Klassifikation der Weichteiltumoren
- Ostitis fibrosa cystica
- extraskeletal musculoskeletal tumors by compartment
- Osteoklastom
- extra skeletal musculoskeletal lesions by compartment
- Sehnenscheidenfibrom
- Riesenzelltumor des Beckenknochens
- giant cell tumour in children
- giant cell tumor of the tendon sheath of the hand
- giant cell tumour of peroneal tendon sheath


 Assoziationen und Differentialdiagnosen zu Riesenzelltumor der Sehnenscheiden:
Assoziationen und Differentialdiagnosen zu Riesenzelltumor der Sehnenscheiden:






