toxic encephalopathy





Toxic leukoencephalopathy is an encephalopathy predominantly affecting white matter as a result of a toxic substance. The presentation can either be chronic or acute. In the acute phase, acute toxic leukoencephalopathy can have a characteristic and profound MR imaging appearance that is potentially reversible with therapy or removal of the offending agent.
Clinical presentation
The clinical presentation of toxic leukoencephalopathy is extremely variable, ranging from minor cognitive impairment, easily confused with psychiatric illnesses, to severe neurological dysfunction. The lack of imaging in patients with minimal or mild encephalopathic symptoms may account for why this entity may be underdiagnosed in the acute phase. Notably, worse outcomes from acute toxic leukoencephalopathy can be seen with opiate-related insults relative to immunosuppression and hepatic/hyperammonemic-related toxic leukoencephalopathy.
Adjunct laboratory testing for confirmation
Myelin basic protein (MBP) is usually elevated in the large majority (>80%), while blood urea nitrogen (BUN) is elevated in the majority (>50%).
Pathology
Etiology
There are numerous agents implicated in toxic leukoencephalopathy. These include:
- antineoplastic drugs
- methotrexate (10% IV, 40% intrathecal)
- carmustine
- cisplatin
- cytarabine
- fludaribine (note: the insult may occur weeks after the exposure)
- fluorouracil (5-FU)
- thiotepa
- interleukin-2 (IL-2)
- interferon alpha (INF alpha)
- immunosuppresive drugs
- cyclosporin
- tacrolimus
- cytoxan
- antimicrobial agents
- amphotericin B
- hexachlorophene
- metronidazole
- drugs of abuse
- toluene
- ethanol
- methanol
- ethylene glycol
- cocaine
- MDMA a.k.a. "ecstasy" (3,4-methylnedioxymethamphetamine)
- intravenous heroin
- inhaled heroin pyrolysate ("chasing the dragon")
- psilocybin (active substance in 'magic mushrooms')
- opiate-derived oral medications in large amounts (overdose)
- environmental toxins
- carbon monoxide (CO)
- arsenic (As)
- carbon tetrachloride (CCl4)
- cranial irradiation
- sepsis
- metabolic abnormalities
- hyperglycemia
- uremia
- hyperammonemia (in the setting of hepatic failure)
The more common of these causes can be remembered with a mnemonic: CHOICES.
Radiographic features
The findings are potentially reversible with therapy or removal of the offending agent in the early phase.
MRI
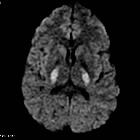
- FLAIR: white matter abnormalities are typically confluent and symmetric, and may involve the corpus callosum as well, particularly the splenium
- DWI: white matter abnormalities are similar to FLAIR, typically confluent and symmetric, and may involve the corpus callosum as well, particularly the splenium
- SWI: in about 15%, there are punctate (<5 mm size) microhemorrhages scattered throughout the periventricular white matter
Siehe auch:
- mikroangiopathische Leukenzephalopathie
- Chasing the dragon
- Kohlenmonoxidintoxikation
- Methotrexat induzierte Leukoenzephalopathie
- cortisol related leukoencephalopathy
- cocaine-related leukoencephalopathy
und weiter:


 Assoziationen und Differentialdiagnosen zu toxic leukoencephalopathies:
Assoziationen und Differentialdiagnosen zu toxic leukoencephalopathies:


