Cerebral microhemorrhage

Hypertensive
microangiopathy • Hypertensive encephalopathy and hypertrophic olivary degeneration - Ganzer Fall bei Radiopaedia

Comparison of
conventional gradient echo T2*-weighted image (left, TE=20ms), susceptibility weighted image (SWI) and SWI phase image (center and right, respectively, TE=40ms) at 1.5 Tesla. Low signal foci in cerebral amyloid angiopathy (CAA) is shown.

Cerebral
microhemorrhage • Multiple cavernoma syndrome - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Immune effector cell-associated neurotoxicity syndrome (ICANS) - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Lymphoma - intravascular - Ganzer Fall bei Radiopaedia

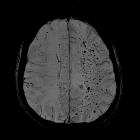
Zahlreiche
zerebrale Mikroblutungen vorwiegend Thalamus und Basalganglien am ehesten als folge einer zerebrale hypertensiven Angiopathie. Oben T2, T1, unten FLAIR, SWI. Die Befunde sind mit Abstand am besten in der suszeptibilitätsgewichteten Sequenz sichtbar.

Susceptibility
weighted image (SWI) of diffuse axonal injury in trauma at 1.5 Tesla. Conventional GRE (left) with TE=20 ms and SWI (right) with TE=20 ms.

Microbleeds
show a characteristic distribution in cerebral fat embolism. A case showing microhemorrhages as seen on CT. Axial native CT scan images at the level of the centrum semiovale and the basal ganglia of a 16-year-old polytraumatised female patient acquired on postoperative day 11 after hospital admission. Multiple subcortical punctiform hyperdensities presumably representing microhemorrhages are seen bilaterally in the subcortical white matter (a), and a larger hyperdensity is seen in the genu of the corpus callosum (b)

Microbleeds
show a characteristic distribution in cerebral fat embolism. A case representing the walnut kernel microbleed pattern. SWI (a–d) MRI images at the level of the centrum semiovale (a), at the level of the corona radiata (b), at the level of the basal ganglia (c), and at the level of the brainstem and the cerebellum (d) of a 16-year-old polytraumatised female patient acquired on day 12 after hospital admission. SWI shows very high number of monotonous punctuate microbleeds in the subcortical white matter, the internal capsule, the corpus callosum, the cerebellum and the brainstem resembling a “walnut kernel”. The larger hypointensity visible in the right centrum semiovale and near the third ventricle is due to a ventricular drain (a–c)

Cerebral
microhemorrhage • Cerebral amyloid angiopathy - Ganzer Fall bei Radiopaedia
Cerebral
microhemorrhage • Radiotherapy induced microhemorrhages - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Parry-Romberg syndrome with intracranial manifestations - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Cerebral fat embolism - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) - Ganzer Fall bei Radiopaedia

Diffuses
axonales Schertrauma bei Motorradunfall. Kontrolle in der MRT nach 3 Tagen: Man erkennt die aus der CCT bekannte kleine balkennahe Blutung in der T1w schon nicht mehr. Gut zu sehen allerdings in FLAIR, DWI und am besten in der T2* (Haem).

Cerebral
microhemorrhage • COVID-19 complicated by leukoencephalopathy and cerebral microhemorrhages - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Posterior reversible encephalopathy syndrome with microhemorrhage (importance of susceptibility-weighted imaging) - Ganzer Fall bei Radiopaedia

Cerebral
microhemorrhage • Amyloid-related imaging abnormalities (ARIA) - Ganzer Fall bei Radiopaedia

Hypertensive
microangiopathy • Chronic hypertensive encephalopathy - Ganzer Fall bei Radiopaedia

Diffuse
axonal injury (grading) • Diffuse axonal injury - Ganzer Fall bei Radiopaedia

Hypertensive
microangiopathy • Chronic hypertensive encephalopathy - Ganzer Fall bei Radiopaedia

Hypertensive
microangiopathy • Chronic hypertensive encephalopathy - Ganzer Fall bei Radiopaedia

Central
nervous system vasculitis • Granulomatous vasculitis - Ganzer Fall bei Radiopaedia
Cerebral microhemorrhages, or cerebral microbleeds, are small focal intracerebral hemorrhages, often only visible on susceptibility-sensitive MRI sequences.
Pathology
Common etiologies
- cavernous malformations
- especially Zabramski classification type IV malformations
- causes include multiple (familial) cavernous malformation syndrome and post-cerebral radiotherapy
- cerebral amyloid angiopathy (common)
- typically involves the grey-white matter junction; usually spares the basal ganglia
- chronic hypertensive encephalopathy (common)
- typically involve the basal ganglia, thalami as well as brainstem, cerebellum and corona radiata
- diffuse axonal injury (DAI) and other trauma
- typically involves the grey-white matter junction, splenium of the corpus callosum, and dorsolateral brainstem
Less common etiologies
- acute hemorrhagic leukoencephalitis (AHLE)
- CADASIL
- microhemorrhages have been reported to occur in 25–70% of cases without a characteristic distribution
- cerebral hyperperfusion syndrome
- cerebral vasculitis (primary or secondary)
- microhemorrhages usually located at the corticomedullary junction
- COL4A1 brain small-vessel disease
- microhemorrhages have been reported in up to 53% of cases, characteristically in the centrum semiovale, deep gray matter, or brainstem
- hemorrhagic micrometastases
- especially melanoma or renal cell carcinoma
- hypoxia (e.g. acute respiratory distress syndrome, high-altitude exposure, being critically ill)
- intracranial embolism:
- fat embolism
- usually from fractures
- gas embolism
- many causes including: intravenous catheter placement, decompression sickness, extracorporeal membrane oxygenation, hydrogen peroxide ingestion, etc.
- septic embolism
- usually from infective endocarditis
- fat embolism
- intracranial infection (e.g. cerebral malaria, mycotic aneurysm)
- intravascular lymphoma
- posterior reversible encephalopathy syndrome (PRES)
- progressive facial hemiatrophy (PFHA)
- radiation-induced cerebral vasculopathy
- thrombotic microangiopathies (e.g. hemolytic uremic syndrome and thrombotic thrombocytopenic purpura)
Radiographic features
Cerebral microhemorrhages are generally only seen on MRI and are best seen on susceptibility weighted T2* sequences such as gradient-recalled echo (GRE) and susceptibility weighted imaging (SWI).
They appear as conspicuous 2-10 millimeter punctate regions of signal drop out with blooming artifact. This blooming grossly overestimates the size of the lesions, and they are usually inapparent on other sequences.
Differential diagnosis
- artificial heart valve metallic emboli (very rare)
- pneumocephalus (very rare without proceeding surgery)
- flow voids of veins
- intracranial calcification
Siehe auch:
- Zerebrale Amyloidangiopathie
- Pneumocephalus
- Kavernom
- Diffuses axonales Schädelhirntrauma
- zerebrale Kavernome
- CADASIL
- zerebrale Mikroangiopathie bei Hypertonus
- Mikroblutungen
- Mikroblutungen in den Basalganglien
- Taucherkrankheit
- Mikroblutungen im Thalamus
- Vaskulitis des Zentralen Nervensystems
- multiple (familial) cavernous malformation syndrome
und weiter:


 Assoziationen und Differentialdiagnosen zu zerebrale Mikroblutungen:
Assoziationen und Differentialdiagnosen zu zerebrale Mikroblutungen:







