uterine artery embolisation




Uterine artery embolization (UAE) is an interventional radiological technique to occlude the arterial supply to the uterus and is performed for various reasons.
History
Uterine artery embolization has been practised for more than 20 years for controlling hemorrhage following delivery/abortion, in ectopic or cervical pregnancy, gestational trophoblastic disease or carcinoma of the cervix.
The technique was first reported as an effective intervention for fibroids in 1995 when Ravina et al noted that several women with symptomatic leiomyomata who underwent uterine artery embolization as a pre-hysterectomy treatment had significant clinical improvement to an extent that hysterectomy was no longer required.
It is now estimated that more than 100,000 UAE procedures may have been performed so far for the treatment of fibroids.
Indications
- intramural fibroids
- menorrhagia
- pelvic pain and pressure symptoms
- bladder outlet obstruction and hydronephrosis due to ureteric compression
- fibroids with otherwise undiagnosed infertility
- as a preoperative measure for large fibroids
- dysfunctional uterine bleeding
- adenomyosis
- other less common indications include
- uterine artery pseudoaneurysm(s)
- uterine AVM: trauma, post curettage
- if active extravasation of contrast is detected during angiography for another reason (post-trauma)
Patients with fibroids, and their related problems, probably present the largest group who is most able to benefit from percutaneous treatment. Presently people with uterine fibroids traditionally undergo total abdominal, vaginal or laparoscopic-assisted hysterectomies around the world. The figure in the United States is about 60,000 hysterectomies per year. In less developed and more populous countries like India, the numbers may be even higher. There is an increasing need for non-invasive or less invasive alternatives for uterine fibroids and dysfunctional bleeding.
Contraindications
- contraindications to angiography
- severe anaphylactoid reaction to contrast media
- uncorrectable coagulopathy
- severe renal insufficiency
- pregnancy
- active pelvic infection
- prior pelvic radiation
- connective tissue disease
- prior surgery with adhesions (relative)
In addition, many international obstetrics practice guidelines acknowledge that the effect of uterine artery embolization (UAE) on pregnancy is understudied and thus currently do not recommend performing UAE on women who maintain a future desire for pregnancy. Exceptions to this may include women who have severe anemia or symptoms associated with fibroids, have failed conservative measures and have contraindications to surgery or those who consent to UAE within an approved research protocol.
Procedure
Preprocedural evaluation
- a thorough evaluation of patients symptoms and signs in consultation with a gynecologist
- pelvic ultrasound and MRI
- Pap smear and endometrial biopsy
- relevant history of other medical problems
- allergies
Equipment
Catheter selection
Any catheter suitable for contralateral and ipsilateral uterine artery cannulation
- Robertson uterine catheter (RUC): commonly used selective catheter for pelvic angiography
- Cobra glidecath: can also be used
- right internal mammary catheter: may be used, but less common
If the above mentioned catheters are not available, bilateral common femoral artery puncture is an option for contralateral access to the uterine arteries.
Embolic agents
The type of embolic agent selected will depend on the indication.
- fibroids
- PVA (300-350 microns)
- embospheres (700 microns for fibroids, 500microns for adenomyosis)
- postpartum hemorrhage or vaginal bleeding
- gel foam slurry
- coils (occasionally)
- n-butyl-cyanoacrylate (glue)
Technique
The approach is dependent on operator preference.
Femoral access:
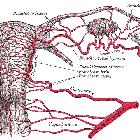
The contralateral internal iliac artery is selected. The uterine artery is a branch of its anterior division and has a distinctive radiographic appearance. Care is taken to avoid cervical and vaginal branches, this is usually avoided by superselective catheterization of the uterine artery distal to the origin of these branches.
The ipsilateral uterine artery is selected by formation of a waltman loop and subsequent embolization performed.
Embolization endpoint is stasis of the main uterine artery trunk.
The ovarian arteries may also be interrogated and if fibroid vascularity is detected these may also be embolized.
Brachial or radial access:
This is performed via the left upper limb. In general, this technique allows for easier uterine artery selection, however, it presents challenges regarding catheter length and there is a theoretical, but small risk of stroke as the catheter crosses the origin of the left vertebral artery.
Peri-procedural care
- patient-controlled analgesia is required following the procedure unless the interventional radiologist chooses to perform a hypogastric nerve block.
- patients are generally required to stay in hospital overnight to ensure adequate pain relief.
- intra-arterial local anesthetic injection has been described, but this has not achieved widespread acceptance.
- IV fluids
- analgesia
- local anesthesia
- antiemetics
- antibiotics
Intravenous fluids, analgesia, antiemetics and antibiotics need to be continued during the postprocedural period.
Complications
- angiography complications
- post-embolization syndrome
- uterine artery dissection
- sepsis is a rare but serious complication and can be difficult to differentiate from post embolization syndrome.
- vaginal expulsion of fibroid tissue
- premature onset menopause is uncommon but has been described in women over the age of 45.
- reproductive complications including increased risk of IUGR, PPH and PROM have been described in women who have undergone embolization. It is unclear how much of this increased risk is attributable to the fibroids themselves or the embolization procedure.
Outcomes
For vaginal bleeding
- alleviates need for emergency hysterectomy
- resumption of menstruation
- successful pregnancy after UAE for postpartum hemorrhage (PPH)
- unsuspected abnormalities treated during UAE for PPH
For fibroids
- menorrhagia/dysmenorrhea and metrorrhagia improve in 70-95% of cases
- hospital stay is rarely >48 hours
- patients are often back to work within 10 days
- no post laparotomy complications
- mean uterine volume reduction by 26-59%
- fibroid volume reduction by 40-75% (at the end of 6 months)
- the overall complication rate is at ~10% with major complications at ~1.5%
In a recent study of two years following therapy, women with symptomatic uterine fibroids were shown to have mildly better health quality of life results with Myomectomy than uterine artery embolization .
Current recommendations
- American College of Obstetrics and Gynecology (ACOG) in 2008 issued guidelines that patients with fibroids may be given an option of uterine artery embolization
- NICE(UK): in 2007 recommended uterine artery embolization with surgery as a first-line treatment option
See also
Siehe auch:
- Uterus
- Leiomyofibrom Uterus
- Adenomyose
- Blasenentleerungsstörung
- arteriovenöse Malformation des Uterus
- Uterusmyom-Embolisation
- Arteria uterina
- uterine artery embolisation : MRI assessment
- nekrotisch verändertes Uterusmyom
- Postembolisationssyndrom
- Uterusatonie
und weiter:


 Assoziationen und Differentialdiagnosen zu Embolisation Arteria uterina:
Assoziationen und Differentialdiagnosen zu Embolisation Arteria uterina: