Varicocele embolization

Zustand nach
Embolisation der Vena testicularis links bei Varikozele. Die Röntgenübersichtsaufnahme des Abdomens zeigt die längs aneinander gereihten, gewundenen Coils in Projektion auf den Psoas.

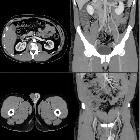
Zustand nach
Embolisation der Vena testicularis links bei Varikozele. In der Computertomographie axial sieht man im Verlauf der Vene vor dem Psoas die metalldichten Coils mit entsprechenden Artefakten.

Varicocele
embolization • Varicocele embolization - Ganzer Fall bei Radiopaedia

Varicocele
embolization • Varicocele embolization with polidokanol and coil - Ganzer Fall bei Radiopaedia

Varicocele
embolization • Amyand hernia with acute appendicitis - Ganzer Fall bei Radiopaedia

Role of
varicocele sclerotherapy in the management of benign prostatic hyperplasia and its associated lower urinary tract symptoms (pilot study). Diagram showing A normal, B pathological and C post sclerotherapy testicular-prostatic venous changes with emphasis on the hydrostatic pressure changes for blood column lengths (EIV = external iliac vein, IIV = internal iliac vein, CIV = common iliac vein)

Role of
varicocele sclerotherapy in the management of benign prostatic hyperplasia and its associated lower urinary tract symptoms (pilot study). A prostatic capsular contrast ‘blush’ (long arrows) following spermatic venous opacification confirms the backdoor phenomenon [7] “Copyright (2022) Wiley. Used with permission from (Gat and Goren, Benign prostatic hyperplasia: Long-term follow-up of prostatic volume reduction after sclerotherapy of the internal spermatic veins, Andrologia, Wiley)” (pp = pampiniform plexus)
Varicocele embolization is a minimally invasive method of treating varicoceles by embolizing the testicular vein (internal spermatic veins).
Indications
- symptomatic varicocele
- infertility/subfertility
- failed surgical ligation
Contraindications
Relative contraindications include:
- intravenous contrast allergy
- renal impairment
- coagulopathy
Preparation
- full clinical assessment including comprehensive medical history, physical examination, lab tests including coagulation profile, renal function, seminal sperm count and scrotal ultrasound should be performed prior to the procedure
- embolization performed on outpatient basis as a day case
- conscious sedation may be required but general anesthesia typically not required
Technique
- metallic coils, detachable balloons, vascular plugs, NBCA glue, sodium tetradecyl sulfate are used for embolization
- may approach from internal jugular vein (IJV) or common femoral vein. Less acute angulation of catheter with IJV approach
- lead shield over testicles
- sheath, angled catheter, microcatheter and guide wire used: products vary according to user preference and availability
Left side
- select left renal vein and perform renal venogram to note location of testicular vein entry point and presence of collateral vessels (Bähren classification of left varicoceles)
- select left testicular vein from left renal vein and perform venogram to note size of vein and presence of collateral veins. The ability to inject contrast retrogradely from the top of the testicular vein down to the groin indicates absent or incompetent valves
- advance catheter to level of superior pubic ramus and insert coils along length of testicular vein in a cephalad direction
- coils should not be inserted below level of inguinal ligament because patient may feel them
- uppermost coil should not project into lumen of renal vein due to risk of renal vein thrombosis
- duplicated testicular veins and collateral draining veins should be occluded otherwise persistent inflow may cause procedural failure. This may be achieved by ensuring coils are placed across point of opening of collateral channel into testicular vein, or by directly entering and embolizing the duplicated or collateral vessel if large enough
- perform post-embolization venogram to ensure successful occlusion of flow
Right side
- right testicular vein is selected from IVC (or, in a small percentage, from right renal vein, a rare anatomical variant)
- otherwise the same procedure as for the left side
Side effects
- back pain or abdominal pain: typically mild and resolves in 24 to 48 hours
Complications
- venous perforation: generally subclinical and self-limiting
- misplacement of coil (e.g. into renal vein): usually retrievable with snare
- embolization of coil into pulmonary circulation (if coil undersized): usually retrievable with snare
- failed embolization: usually due to patent venous collaterals
Post-procedure management
- remove catheter and sheath and secure hemostasis at puncture site
- observe for 1 to 4 hours
Outcomes
- outcome almost identical for embolotherapy and surgical ligation
- technical success rate close to 100%
- pregnancy rate approximately 35%
Advantages
- minimally invasive
- day procedure
Disadvantages
- pregnancy rate much lower than technical success rate, but the same as for surgery
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Varicocoele embolization:
Assoziationen und Differentialdiagnosen zu Varicocoele embolization: