testicular and scrotal ultrasound








Testicular and scrotal ultrasound is the primary modality for imaging most of the male reproductive system. It is relatively quick, relatively inexpensive, can be correlated quickly with the patient's signs and symptoms, and, most importantly, does not employ ionizing radiation.
MRI is occasionally used for problem solving if the diagnosis is unclear on ultrasound. CT is only rarely needed, and is avoided because of its ionizing radiation. Nuclear medicine studies (e.g. Tcm-pertechnetate) have also fallen out of favor because of their ionizing radiation.
Normal ultrasound anatomy
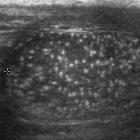
Testis
- homogeneous echogenicity
- a prepubertal testis has a slightly decreased echogenicity relative to an adult
- mildly coarse echotexture
- adult diameter measures between 3-5 cm, with a volume of ~20 mL
- the tunica (vaginalis/albuginea) appears as an echogenic outline of the testicle:
- the tunica invaginates to form the linear echogenic testicular mediastinum (a.k.a. mediastinum testis)
- the rete testis can be identified in ~20% of patients
- hypoechoic region near the mediastinum
- more noticeable if dilated
- appendix testis: attached to upper pole of testicle, near the epididymis
- not usually seen unless torsion is present
- spectral Doppler: the testis demonstrates a low-resistance arterial waveform
Epididymis
- epididymal head: round or oblong structure located near the superior pole of the testicle
- isoechoic or mildly hyperechoic relative to the testicle
- measures 5-12 mm
- epididymal body: extends down the posterior aspect of the testicle
- measures 2-4 mm
- epididymal tail: curved structure at the inferior pole of the testicle and becomes the proximal ductus deferens
- measures 2-5 mm
- appendix epididymis: attached at the epididymal head
- not normally seen unless torsion present
- spectral Doppler: epididymis demonstrates a low-resistance arterial waveform
Scrotum
- normal scrotal skin thickness varies between 2-8 mm
Technique
A high-frequency transducer (9-15 MHz) is usually used for evaluation of the testes and scrotum, except in certain circumstances (e.g. massive hydrocele), when a lower MHz transducer is used.
- patient is supine
- patient may be upright when looking for an inguinal hernia
- scrotum is supported on a towel laid over the thighs
- testicles should be evaluated in both long and short axes
- if a scrotal mass is found, one of the primary roles of ultrasound is to determine if it is intratesticular or extratesticular
- intratesticular mass: generally malignant
- extratesticular mass: 3-6% malignant
- if a scrotal mass is found, one of the primary roles of ultrasound is to determine if it is intratesticular or extratesticular
- color and spectral Doppler parameters should be set for low flow
- low wall filter and low pulse repetition frequency
- power Doppler may be necessary to prove testicular torsion
- important: both a short axis grayscale and a color Doppler image should be obtained, in which both testicles are imaged side-by-side ("buddy shot" or "sunglasses view"), to compare the size, relative echogenicity and blood flow
- scrotum should be examined for extratesticular masses or processes
Tips:
- use enough gel to eliminate gas trapped in the skin folds of the scrotum
- do not change the setting when moving from one testicle to the other
See also
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Sonographie des Skrotums und Hodens:
Assoziationen und Differentialdiagnosen zu Sonographie des Skrotums und Hodens: