hypoparathyroidism
Hypoparathyroidism:Case
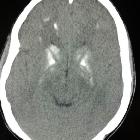
report. Unenhanced axial sections through the brain showing bilateral symetrical basal ganglia calcifications

Hypoparathyroidism:Case
report. T1 hyperintense signals in bilateral basal ganglia

Hypoparathyroidism:Case
report. T2* image through brain showing drop out signals in bilateral basal ganglia, corresponding to calcifications seen on CT

Falx
ossification • Chronic secondary hypoparathyroidism - Ganzer Fall bei Radiopaedia

Toddler with
developmental delay who had a seizure and fell on the floor. Axial (above) and coronal (below) CT without contrast of the brain shows multiple bilateral calcifications in the subcortical white matter. There are additional CSF spaces present between the leaflets of the septum pellucidum and anterior to the splenium of the corpus callosum.The diagnosis was hypoparathyroidism in a patient with cavum septum pellucidum and cavum vergae.
Hypoparathyroidism results from reduced secretion of parathyroid hormone by the parathyroid glands. It results in hypocalcemia.
Epidemiology
Hypoparathyroidism has an estimated prevalance 37 per 100,000 person-years and incidence of 0.8 per 100 000 person-years. It carries no increased risk of mortality. The majority of cases are due to complications from anterior neck surgery.
Clinical presentation
- tetany: peripheral paresthaesia, carpopedal spasm, seizures
- emotional lability, depression and anxiety, psychosis
- short stature
Pathology
There are a number of causes of hypoparathyroidism :
- iatrogenic, e.g. post parathyroidectomy or thyroidectomy
- congenital absence of the parathyroid glands, which may be syndromic in thymic aplasia, or 22q11.2 deletion syndrome (a.k.a. DiGeorge syndrome)
- familial, e.g. autoimmune polyendocrine syndrome type 1
- idiopathic (probably autoimmune-mediated destruction)
Markers
- parathyroid hormone (PTH) level: low
- serum phosphate level: high
- serum calcium level: low
Radiographic features
- musculoskeletal
- focal (~25%) and generalized (~10%) osteosclerosis
- dense metaphyseal bands
- skull vault thickening
- diffuse idiopathic skeletal hyperostosis-like changes
- subcutaneous calcification (around shoulders and hips)
- CNS
- intracranial calcifications: most commonly basal ganglia but also subcortical white matter, corona radiata and thalamus
- head and neck
Differential diagnosis
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Hypoparathyreoidismus:
Assoziationen und Differentialdiagnosen zu Hypoparathyreoidismus:
