intrahepatische Cholelithiasis
intrahepatische Cholelithiasis
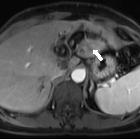
Cholezystolithiasis Radiopaedia • CC-by-nc-sa 3.0 • de
Gallstones, also called cholelithiasis, are concretions that may occur anywhere within the biliary system, most commonly within the gallbladder.
Terminology
Gallstones (cholelithiasis) describe stone formation at any point along the biliary tree. Specific names can be given to gallstones depending on their location:
- cholecystolithiasis: gallstones within the gallbladder
- the terms cholelithiasis or gallstones have been largely used in clinical practice by their own to refer to stones in the gallbladder
- choledocholithiasis: gallstones within the bile ducts
Biliary microlithiasis refers to gallstones <3 mm in diameter. The term biliary microlithiasis is occasionally used as a synonym for sludge, however, this is not strictly correct. Sludge may include these microliths in its composition, but these are only one element of a variable mixture of crystals, proteinaceous debris, lysed cells and mucin .
Epidemiology
Gallstones occur in ~10% of the population with a predominance in women (F: M = 2:1). The prevalence increases with age in both sexes .
Genetics may have an important role in gallstone formation. Several studies have shown an association between age-adjusted prevalence of gallstone, ethnicity and family history of gallstones:
- highest age-adjusted prevalence (~50%): Pima Indians, some North and South American Indians
- intermediate age-adjusted prevalence (up to 20%): Caucasians (20%), and Asian population (5-20%)
- lowest age-adjusted prevalence (≤5%): Africans
Risk factors
Common risk factors for cholesterol gallstones include:
- female sex
- middle age
- obesity
- positive family history
- recent rapid weight loss
Also see 5-F rule.
Clinical presentation
Gallstones may be symptomatic in only 25% of cases. The most common presentation is with biliary colic (right upper quadrant or epigastric abdominal pain or discomfort, especially after a fat-rich meal). Other symptoms include belching, bloating, flatulence, heartburn, and nausea.
Abdominal pain is often referred to the right shoulder. Patients may demonstrate this radiation to the tip of the scapula by placing their hand behind the back and thumb pointing upwards: "Collins sign". This may be useful in distinguishing gallstone pain from esophagitis, gastritis, or duodenal ulcer in ~50% of patients .
Pathology
There are three types of gallstones :
- cholesterol (10%)
- >50% cholesterol contents; form with supersaturation of bile, nucleation and stone growth
- predisposing factors
- diet, sedentary lifestyle, the rapid loss of weight, obesity, oral contraceptive pill, total parenteral nutrition (TPN)
- ethnicity, genetic predisposition, older age, female sex
- mixed (80%)
- 20-50% cholesterol content
- predisposing factor: similar to cholesterol stones
- pigment stones (10%)
- <20% cholesterol content; high bilirubin content and occur when there is supersaturation of unconjugated bilirubin
- two further subtypes each with their own predisposing factors:
- black pigment stones: chronic hemolysis, liver cirrhosis, intestinal malabsorption (e.g. Crohn disease)
- brown pigment stones: bacterial infection, parasitic infection (e.g. Clonorchis sinensis) and biliary stasis
Complications
- biliary colic
- cholecystitis
- acute cholangitis
- pancreatitis
- obstructive jaundice
- gallbladder empyema
- gallbladder hydrops/mucocele
- cholecystoduodenal fistula leading to a gallstone ileus or Bouveret syndrome
- Mirizzi syndrome
- increased risk of cholangiocarcinoma
Radiographic features
Plain radiograph
Some radiopaque gallstones may be seen on plain film:
- gallstones are radiopaque only in 15-20% of cases
- may be laminated (a.k.a. lamellated): radiopaque outline with lucent center
- may have a faceted outline
- may show a Mercedes-Benz sign: triradiate pattern of gas lucency
Ultrasound
Ultrasound is considered the gold standard for detecting gallstones :
- greyscale ultrasound
- highly reflective echogenic focus within gallbladder lumen, normally with prominent posterior acoustic shadowing regardless of pathological type (acoustic shadowing is independent of the composition and calcium content)
- gravity-dependent movement is often seen with a change of patient position (the rolling stone sign)
- color Doppler
- may demonstrate a twinkling artifact and is particularly useful for identification of small stones
CT
Calcified gallbladder stones are hyperattenuating to bile, making them the only type to be clearly visualized on CT scan images. Pure cholesterol stones are hypoattenuating to bile, and other gallstones are isodense to bile and these may not be clearly identified on CT.
MRI
- T1-weighted 3D fast spoiled gradient echo (3D FSPGR):
- pigmented stones (hyperintense)
- cholesterol stones (hypointense)
- T2: signal void or low signal outlined by markedly hyperintense bile within the gallbladder
- MRCP: focus of signal void inside the gallbladder
Differential diagnosis
Possible imaging differential considerations in selected situations include
- ingested iron tablets (pseudogallstones) on plain radiograph
- gallbladder polyp
- echogenic bile (sludge) and tumefactive sludge: non-shadowing
- gallbladder carcinoma
Practical points
- gallstone acoustic shadowing is prominent with
- larger size stones (usually >3 mm for shadowing)
- higher transducer frequency
- focal zone at the level of gallstone
- a gallbladder full of stones may paradoxically be hard to visualize (wall-echo-shadow sign)
Siehe auch:


 Assoziationen und Differentialdiagnosen zu intrahepatische Cholelithiasis:
Assoziationen und Differentialdiagnosen zu intrahepatische Cholelithiasis:

