Meckeldivertikulitis

















Meckel diverticulitis is the inflammation of Meckel diverticulum, which is the most common congenital structural abnormality of the gastrointestinal tract . Despite this, it is an uncommon cause of acute abdomen and is often not correctly diagnosed pre-operatively.
This article focuses on Meckel diverticulitis. For a general discussion of the un-inflamed diverticulum, please refer to the article on Meckel diverticulum.
Epidemiology
Meckel diverticulum is seen in approximately 2% of the adult population and among those with symptoms, males are disproportionately affected compared to females in a ratio of 2-4:1 .
Clinical features
Patients usually present with acute pain in the right lower quadrant. Painless rectal bleeding is also frequent.
Pathology
A number of mechanisms are recognized as precipitants of diverticulitis. Meckel diverticulitis can occur due to bacterial infection, which can go on occasionally to gangrene. This is similar in pathogenesis to acute appendicitis or colonic diverticulitis.
Peptic ulceration due to acid secretion from gastric mucosa (see Meckel diverticulum) or diverticular torsion is also encountered.
Radiological features
Ultrasound
Meckel's diverticula are usually seen as a tubular incompressible blind-ending hypoechoic structure with irregular margins. Occasionally it may also be seen as a cyst, raising a different differential diagnosis of intestinal duplication which however is said to have regular margins . Doppler may reveal anomalous vessels and signs of inflammation along the diverticulum.
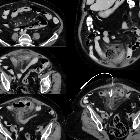
CT
CT is the main modality employed in imaging patients with acute abdominal pain and signs of inflammation.
Meckel diverticula are round or tubular fluid/air-filled structures communicating with small bowel with a wall-to-wall diameter of 1.5-6 mm. Mural wall thickening and enhancement are seen with surrounding inflammatory changes in the adjacent fat as well as small reactive mesenteric lymph nodes. Wall enhancement will be absent in gangrenous Meckel diverticulum.
Rarely, an enterolith can also be visualized within the diverticulum. As is the case with appendicitis, it is said that contrast opacification of diverticula is suggestive of inflammation.
Small bowel obstruction may also be present and in many cases, this is the only pre-operative finding.
Reporting checklist
Identification of Meckel diverticulitis requires not only familiarity with the condition but also a careful examination of the small bowel. If an inflamed diverticulum is identified a number of features should be sought and commented upon, including:
- diverticulum
- estimate the distance from the ileocecal junction
- size/length of the diverticulum
- location relative to the abdominal surface anatomy
- enhancement/non-enhancement of the wall (non-enhancement suggests gangrene and impending rupture)
- appendix: look for signs of inflammation
- free intra-abdominal gas
- intra-abdominal fluid/abscess formation
- small bowel obstruction
Nuclear medicine
Tc-99m pertechnetate scan
Ectopic gastric mucosa, if present, can be picked up on this scan, but it does not usually play a role in the acute presentation.
Differential diagnosis
Clinically the differential diagnosis is broad, and unless a Meckel diverticulum is known to be present, Meckel diverticulitis is usually not specifically suspected.
Imaging can also be challenging, with the most common differentials including:
- acute appendicitis
- identifying a normal appendix is thus crucial
- terminal ileitis
- Crohn disease
- typhilitis
- infective terminal ileitis
- omental infarction
- epiploic appendagitis
- intestinal lumen may be inflamed but retains normal contour
- rounded fat density nodule with central hyperdense dot
- intestinal duplication: usually has regular margins, whereas Meckel diverticula have irregular margins.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Meckeldivertikulitis:
Assoziationen und Differentialdiagnosen zu Meckeldivertikulitis: