Acute abdominal pain
Acute abdominal pain is a common acute presentation in clinical practice. It encompasses a very broad range of possible etiologies and diagnoses, and imaging is routinely employed as the primary investigative tool in its modern management.
Terminology
A subgroup of patients with acute abdominal pain will have a so-called acute abdomen (also known as an acute surgical abdomen). This is restricted to those with an acute presentation of abdominal pain coupled with serious morbidity, a tender abdomen and marked rigidity (a.k.a. involuntary guarding) on abdominal physical examination.
Epidemiology
It is estimated that approximately 5% presentations to a typical emergency department are for acute abdominal pain .
Clinical presentation
Acute abdominal pain includes a wide spectrum of severity and differing character, with qualifying descriptors, such as sharp, colicky, dull, etc.
Pathology
Etiology
The list of causes of acute abdominal pain is extremely long, and can be subdivided in a multiplicity of ways.
Common causes
- acute visceral inflammation
- bowel obstruction
- bowel ischemia
- acute diverticulitis
- biliary colic
- renal colic
- pyelonephritis
- peptic ulcer disease: gastric or duodenal ulcer
- abdominal aortic aneurysm (AAA)
- inflammatory bowel disease
- mesenteric adenitis
- pregnancy: sometimes it maybe 'concealed', i.e. patient may not even be aware!
Less common causes
- Meckel diverticulitis
- psoas abscess
- rectus sheath hematoma
- spontaneous splenic rupture
- epiploic appendagitis
- omental infarction
Gynecological
- ovarian torsion
- salpingitis
- tubo-ovarian abscess
- ruptured ectopic pregnancy
- uterine rupture
- uterine perforation
Trauma
- penetrating abdominal injury
- blunt abdominal injury
Iatrogenic
- post-operative
- medications
- radiotherapy
Medical causes
Many medical conditions can present with an acute abdominal pain. In some cases it may be an atypical presentation of a common condition (e.g. myocardial ischemia), or a typical presentation of a rare condition (e.g. porphyria). This list is not exhaustive.
- thoracic
- infection
- gastroenteritis: many organisms
- acute hepatitis
- intestinal anthrax
- pneumococcal peritonitis
- shingles (herpes zoster)
- urinary tract infection (UTI)
- tuberculosis
- malaria
- typhoid fever
- cholera
- tabes dorsalis
- infectious mononucleosis: splenic rupture
- endocrine
- diabetes mellitus
- pheochromocytoma
- thyrotoxic crisis (thyroid storm)
- musculoskeletal
- epidemic myalgia
- abdominal muscle injury e.g. rectus abdominis muscle strain
- Cyriax syndrome
- vasculitis
- miscellaneous
- sickle cell disease: acute crisis
- lead toxicity
- opiate withdrawal: classically heroin
- porphyria
- selenosis
Functional GI disorders
- functional dyspepsia
- irritable bowel syndrome (IBS)
- functional abdominal pain syndrome
- functional gallbladder disorder
- opioid bowel syndrome
Radiographic features
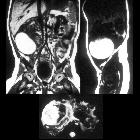
CT of the abdomen and pelvis is the first-line investigation for many presentations of acute abdominal pain. Traditionally, the plain abdominal radiograph was the initial investigation but has fallen out of favor due to its poor sensitivity and specificity for many of the causes of abdominal pain.
Plain radiograph
Historically the plain abdominal radiograph was mandatory in every patient presenting with an acute abdomen.
CT/US/MRI
to be completed
Treatment and prognosis
In the pre-CT era, patients with an acute abdomen were often sent for urgent surgery. Contemporaneously, with the virtually ubiquitous availability of CT, some of these patients will not be operated on at all. Conversely, some patients who do not meet the traditional criteria for an "acute abdomen" will be diagnosed on imaging with conditions, such as acute appendicitis, and be sent for surgery.
Practical approach
A pragmatic approach needs to be taken by clinicians/radiologists when considering the potential causes of an acute abdomen and a surgical sieve may be helpful as a starting point.
Beware of a normal abdominal radiograph providing a false sense of security. Emergent pathologies including bowel obstruction and perforation may not produce a radiographic abnormality.
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Akutes Abdomen:
Assoziationen und Differentialdiagnosen zu Akutes Abdomen: