colonic diverticulitis









































Colonic diverticulitis (plural diverticulitides), is a complication of colonic diverticulosis, and one of the presentations of diverticular disease. Differentiating one from the other is critical since uncomplicated diverticulosis is mostly asymptomatic and acute diverticulitis is a potentially life-threatening illness.
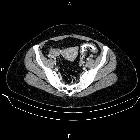
On imaging, non-complicated diverticulitis is characterized by focal fat stranding adjacent to a colonic diverticulum, usually the sigmoid. A small amount of extraluminal fluid and gas locules may be present.
Epidemiology
Diverticulitis is a complication of diverticulosis, and the demographics of the condition are therefore similar, with elderly patients being most at risk. Of those with diverticulosis, 4% will go on to develop diverticulitis .
Clinical presentation
Symptoms of colonic diverticulitis usually begin in the left iliac fossa with unremitting pain and accompanying tenderness. The pain is accompanied by a fever, leukocytosis, and change in bowel movements . An ill-defined mass may also be palpable representing the inflammatory phlegmon. Clinical evaluation alone may be insufficient in the initial diagnosis of diverticulitis and radiological evidence of inflammation is necessary for definitive diagnosis .
As the disease progresses and becomes more generalized (stage III and IV - see Hinchey classification of acute diverticulitis), signs and symptoms also become widespread and indistinguishable from other causes of generalized peritonitis.
Pathology
Colonic diverticular development is thought to involve bowel wall abnormality, increased intraluminal pressure, and lack of dietary fiber . The sigmoid colon has the highest intraluminal pressure and the narrowest caliber, it is therefore the most common site of diverticula formation . Diverticulitis is the result of obstruction of the neck of the diverticulum, with subsequent inflammation, perforation, and infection . Early changes of local inflammatory phlegmon may later progress to abscess formation and generalized peritonitis.
Radiographic features
Although CT is the modality of choice for the diagnosis and staging of colonic diverticulitis with a sensitivity of 94% and specificity of 99%, a dedicated ultrasound study may be able to confidently characterize this condition .
Ultrasound
- diverticula are characterized as bright bowel outpouching (also referred as bowel bright “ears”) showing some degree of acoustic shadowing due to the presence of gas or inspissated feces
- echogenic and non-compressible fat suggesting an inflammatory process of the surrounding fat planes
- thickened bowel wall (>4 mm)
- presence of organized collections imply abscess and thus complicated diverticulitis, which requires further CT assessment
CT
- pericolic stranding, often disproportionately prominent compared to amount of bowel wall thickening
- segmental thickening of bowel wall
- enhancement of colonic wall
- usually has inner and outer high-attenuation layers, with a thick middle layer of low attenuation
- diverticular perforation
- extravasation of gas and fluid into pelvis and peritoneal cavity
- abscess formation (seen in up to 30% of cases)
- may contain fluid, gas or both
- fistula formation (usually a chronic complication)
- gas in the bladder
- direct visualization of a fistulous tract
Treatment and prognosis
Treatment depends on a host of factors, especially patient co-morbidities and stage of the disease.
For localized disease (stage I and II) conservative management with IV antibiotics and rehydration usually suffices. If the first attack of diverticulitis is treated successfully without surgery, most patients do not go on to have further episodes (66-75%). But some have multiple repeated attacks and go on to require surgery.
If the abscess is large, then percutaneous drainage under CT or US may be beneficial (successful in 70-90% of cases) .
Complications
Recognized complications include :
- abscess formation
- fistula formation
- bladder: colovesical fistula
- vagina: colovaginal fistula
- bowel: coloenteric fistula or colocolic fistula
- skin: colocutaneous fistula
- small bowel obstructions from adhesions or bowel wall edema
- perforation resulting in pneumoperitoneum, peritonitis, and sepsis
- pylephlebitis
Surgical treatment
Surgery is the treatment of choice in patients:
- who progress to stage III or IV
- who fail medical management
- in whom carcinoma cannot be excluded
- who have multiple (2 or more) attacks
- who develop fistulas
Surgical options depend on whether surgery is elective or emergent and on the quality of bowel preparation. For elective surgery, the aim is to perform a single-stage segmental colectomy (usually sigmoid colectomy) with a primary end to end anastomosis. In emergent cases, either on-table lavage with primary anastomosis or a two-stage procedure is performed. The two-stage procedure consists of a Hartmann colectomy with end colostomy and rectal stump closure, which is subsequently closed by a second operation. This carries a mortality of less than 5% .
Differential diagnosis
General imaging differential considerations include:
- colorectal carcinoma
- less inflammatory change
- usually shorter segment
- acute appendicitis (for right-sided disease)
- younger patients
- no predilection for Asian patients
- epiploic appendagitis
- ischemic colitis
- pseudomembranous colitis
- bowel wall thickening more pronounced than the amount of stranding
- inflammatory bowel disease
- bowel wall thickening more pronounced than the amount of stranding
- tubo-ovarian abscess
Siehe auch:
- Appendicitis epiploica
- Sigmadivertikulitis
- Divertikulitis
- Sigmadivertikulose
- Kolondivertikulose
- Endometriose des Colon sigmoideum
- intramuraler Abszess
- Divertikulitis Klassifikation nach Hansen und Stock
- Sigmakarzinom
- acute diverticulitis
- Divertikulitis des Zökums
und weiter:


 Assoziationen und Differentialdiagnosen zu Kolondivertikulitis:
Assoziationen und Differentialdiagnosen zu Kolondivertikulitis: 


