mesenteriale Pannikulitis






















Sclerosing mesenteritis, also referred to as mesenteric panniculitis or retractile mesenteritis, is an uncommon idiopathic disorder characterized by chronic non-specific inflammation involving the adipose tissue of the bowel mesentery.
Epidemiology
Typically this condition afflicts adults in their sixties with mild male predilection, although reports vary .
Clinical presentation
Clinical presentation can be variable with abdominal pain, intestinal obstruction or ischemia, a mass, or diarrhea. Altered bowel habits, and weight loss may be present in some cases. Occasionally, intermittent partial bowel obstruction is encountered . A firm left upper quadrant / central abdominal mass may be felt . In some situations sclerosing mesenteritis is asymptomatic.
Pathology
The small bowel mesentery is affected in most cases although the sigmoid mesocolon and omentum can also occasionally be involved.
The disease is said to pass through three stages, although some authors believe these to be separate entities :
Macroscopic appearance
Macroscopically, the mesentery is thickened with either solitary or multiple focal masses .
Histology
Histology demonstrates :
Associations
Numerous associated conditions have been variably described including :
- malignancy
- systemic lymphoma (up to 10% risk of developing lymphoma)
- gastric carcinoma
- recent abdominal surgery
- systemic inflammatory conditions
- autoimmune conditions (may be related to IgG4-related disease)
- may be related to Weber-Christian disease
There is debate about the association between systemic inflammatory conditions and mesenteric panniculitis. Determining causation is difficult. The term "secondary mesenteric panniculitis" is reserved by some authors for patients with systemic inflammatory conditions. Most authors would not use the term when there is a local cause for mesenteric inflammation.
Radiographic features
Ultrasound
Ultrasound typically demonstrates distortion and thickening of the root of the mesentery with a slight decrease in echogenicity. Mass effect may be evident . A halo of sparing around vessels may be also seen on ultrasound as a region of hyperechoic fat . Color Doppler interrogation may show non-deviated mesenteric vessels within the mass .
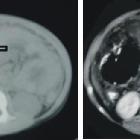
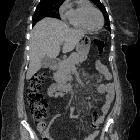
CT
CT features are somewhat dependent on the main tissue component and include:
- well-demarcated or ill-defined mesenteric mass-like lesion with surrounding "misty" attenuation
- "misty" soft-tissue attenuation
The mesentery demonstrates mass effect and may have a ground glass opacity (misty mesentery). Typically the traversing mesenteric vessels and soft tissue nodules have a spared fat halo (this has sometimes been referred to as the fat ring sign). Its orientation is aligned with the root of the jejunal mesentery. Punctate/coarse calcifications (~20%), as well as small lymph nodes (usually <5 mm), may be present within the region.
MRI
Findings are similar to CT. One report described a fibrous capsule around the inflammation .
Nuclear medicine
FDG PET-CT
May have high accuracy for the differentiation between
- sclerosing mesenteritis (or one of its stages): not FDG-avid
- malignant mesenteric involvement: FDG-avid
especially in patients with lymphoma . If in doubt, biopsy may be indicated in selected patients, even in asymptomatic lesions .
Treatment and prognosis
The mainstay of treatment is supportive, as the disease is typically self-limiting. If severe or protracted medical therapy with corticosteroids, cyclophosphamide or azathioprine can be contemplated . Mesenteric panniculitis cannot be completely resected and surgery is of no benefit. In up to 15% of cases, local lymphoma eventually develops . Some authors suggest associated malignancy rate of approximately 56% .
History and etymology
It was first described by Jura in 1924 as “retractile mesenteritis” and further labeled as “mesenteric panniculitis” by Odgen later in the 1960s.
Differential diagnosis
General imaging differential considerations include:
- mesenteric carcinoid tumor
- mesenteric lymphadenopathy due to malignancy:
- lymphoma
- colorectal carcinoma
- carcinoid
- metastatic disease
- mesenteric lymphadenopathy due to inflammation:
- appendicitis
- colonic diverticulitis
- cholecystitis
- pancreatitis
- systemic illness
- mesenteric lipoma: especially if large and if there are lymph nodes within it
- intraperitoneal focal fat infarction
Siehe auch:
- Infarkt des Omentum majus
- Pankreatitis
- Kolorektales Karzinom
- Karzinoid
- Appendizitis
- Cholezystitis
- Tuberkulose des Peritoneums
- Kolondivertikulitis
- Neoplasien des Mesenteriums
- diffuse mesenteriale Flüssigkeitseinlagerungen (misty mesentery sign)
- Pseudomesenteritis
und weiter:
- Appendicitis epiploica
- peritoneales Mesotheliom
- fat halo sign in abdominal CT imaging
- fat halo sign of mesenteric panniculitis
- fat halo sign of inflammatory bowel disease
- fat ring sign
- Mesenteritis
- Gewebsreaktion Fett Bauchraum
- Pannikulitis
- mesenteric panniculitis associated with abdominal tuberculous lymphadenitis


 Assoziationen und Differentialdiagnosen zu mesenteriale Pannikulitis:
Assoziationen und Differentialdiagnosen zu mesenteriale Pannikulitis:







