Blake's-Pouch-Zyste







Blake's pouch cyst is a cystic appearing structure that represents posterior ballooning of the inferior medullary velum into the cisterna magna, below and posterior to the vermis, that communicates with an open fourth ventricle. It is caused by a failure of the regression of Blake's pouch secondary to the non-perforation of the foramen of Magendie.
Epidemiology
It is a rare and underdiagnosed entity .
Clinical presentation
It can present:
- in childhood or adulthood with signs of hydrocephalus (usually headache, vomiting, blurred or double vision)
- later in life or be even asymptomatic, probably due to adequate CSF flow through lateral foramina of Luschka
Pathology
Blake’s pouch, also known as the rudimental fourth ventricular tela choroidea, is a normal transient structure that regresses during embryological development, usually by 12 weeks' gestation, when it starts fenestrating to form the foramen of Magendie (which forms up to the fourth month of gestation).
Persistent Blake's pouch cysts occur due to failed perforation of the foramen of Magendie. As the foramina of Luschka open later than the foramen of Magendie during the embryologic development, this non-perforation of the foramen of Magendie causes enlargement of the ventricular system until the foramina of Luschka open and establishes a precarious compensation via CSF flowing into the cisterns .
Blake's pouch cysts used to be classified as part of the Dandy-Walker continuum, however, this entity is not related to cerebellar or fourth ventricle malformations .
Radiographic features
MRI
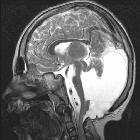
MRI is the imaging modality of choice due to its capacity to differentiate this entity from other posterior fossa malformations. Features include:
- infravermian cyst that communicates with fourth ventricle
- cyst is smooth with thin walls that can be visualized on thin sagittal T2 images
- it can impress on medial side of cerebellar tonsils due to size
- cyst does not communicate with the cisterna magna posteriorly
- upward displacement of the vermis
- no vermian hypoplasia or rotation
- usually hydrocephalus involving the fourth ventricle and supratentorial ventricles (tetraventricular hydrocephalus)
- elevation of the tentorium but usually normally positioned torcula
- choroid plexus can extend from the fourth ventricle into the superior portion of the cyst, which is essentially a ventricular diverticulum
Treatment and prognosis
Preferable treatment of hydrocephalus is endoscopic third ventriculostomy. The prognosis is good after treatment.
History and etymology
It is named after Joseph A. Blake (1864-1937), an American physician who studied the physiology related to the foramen of Magendie .
It was first described as an independent entity within the Dandy-Walker complex in 1996 by Paolo Tortori-Donati et al. .
Differential diagnosis
It needs to be distinguished from other causes of enlarged retrocerebellar "CSF" spaces:
- mega cisterna magna: communicates freely with both fourth ventricle and subarachnoid space
- other entities of the Dandy-Walker continuum: cerebellar vermis malformations
- arachnoid cyst: no hydrocephalus
Siehe auch:
- Mega Cisterna magna
- Arachnoidalzysten der hinteren Schädelgrube
- Blake’s pouch
- Kleinhirnatrophie
- epidermale Inklusionszyste
- Dandy-Walker-Syndrom
- Kleinhirnhypoplasie
- Dandy Walker continuum
- zerebelläre Anomalien
- Zytomegalievirus
- zystische Malformationen der hinteren Schädelgrube
- erweiterter retrocerebellärer Liquorraum
- pädiatrische Erkrankungen des Liquorsystems
und weiter:


 Assoziationen und Differentialdiagnosen zu Blake's-Pouch-Zyste:
Assoziationen und Differentialdiagnosen zu Blake's-Pouch-Zyste: