adnexal torsion

























































Ovarian torsion, also sometimes termed adnexal torsion or tubo-ovarian torsion, refers to rotation of the ovary and portion of the fallopian tube on the supplying vascular pedicle.
It can be intermittent or sustained and results in venous, arterial and lymphatic stasis. It is a gynecological emergency and requires urgent surgical intervention to prevent ovarian necrosis.
Epidemiology
Ovarian torsion has a bimodal age distribution occurring mainly in young women (15-30 years) and post-menopausal women. Approximately 20% of the cases occur during pregnancy .
Torsion occurs due to two main reasons :
- hypermobility of the ovary: <50%
- adnexal mass: ~50-80%
- most lesions are dermoid cysts or paraovarian cysts
- large cystic ovaries undergoing ovarian hyperstimulation are at particular risk
- masses between 5-10 cm are at most risk
Clinical presentation
Most patients present with severe non-specific lower abdominal and pelvic pain, either intermittent or sustained, nausea, and vomiting. There is an adnexal tenderness. A raised white cell count is common.
Pathology
The result of vascular compromise secondary to ovarian torsion is hemorrhagic infarction and necrosis, that can occur as rapidly as within hours of torsion onset.
Torsion of a normal ovary more commonly occurs in young children when developmental abnormalities predispose the ovary to torsions, such as excessively long Fallopian tubes or an absent mesosalpinx.
In adulthood, causes include both benign and malignant ovarian tumors, polycystic ovaries and adhesions. In early pregnancy, a torsion can occur secondary to a corpus luteal cyst or laxity of the adjacent tissues.
Radiographic features
The main feature of torsion is ovarian enlargement due to venous/lymphatic engorgement, edema, and hemorrhage. Secondary signs include free pelvic fluid, an underlying ovarian lesion, reduced or absent vascularity and a twisted dilated tubular structure corresponding to the vascular pedicle. Adnexal torsion is commonly unilateral, with a slight (3:2) right-sided predilection (presumably due to the protective effects of the sigmoid colon on the left) .
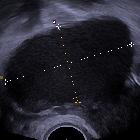
Ultrasound
Ultrasound is the initial imaging modality of choice. Sonographic features include
- enlarged (>4 cm) ovary
- variable echogenicity (hypo- or hyperechoic)
- a long-standing infarcted ovary may have a more complex appearance with cystic or hemorrhagic degeneration
- peripherally displaced follicles with hyperechoic central stroma
- midline ovary position
- free pelvic fluid may be seen in >80% of cases
- an underlying ovarian lesion may be seen (possible lead point for torsion)
- Doppler findings in torsion are widely variable
- little or no ovarian venous flow (common; sensitivity of 100% and specificity of 97%)
- absent arterial flow (a less common, sign of poor prognosis)
- absent or reversed diastolic flow
- normal vascularity does not rule out intermittent torsion
- normal Doppler flow can also occasionally be found due to dual supply from both the ovarian and uterine arteries
- whirlpool sign of twisted vascular pedicle
- ovary tenderness to transducer pressure
- follicular ring sign16
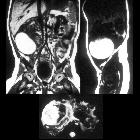
CT
- good at ruling out ovarian torsion if a normal ovary/adnexa is seen on ultrasound
- the twisted ovarian pedicle is pathognomonic for ovarian torsion if demonstrated
- torsion appears as a complex adnexal lesion representing
- enlarged ovary (>4.0 cm )
- distended pedicle
- possible underlying ovarian lesion
- HU >50 on non-contrast CT suggests hemorrhagic necrosis
- lack of enhancement may be seen
- surrounding fat stranding, edema, and free fluid
MRI
Not the imaging modality of choice if torsion is suspected, as urgent imaging is required.
If hemorrhagic infarction is present, signal changes include :
- T1
- thin rim of high signal (methemoglobin) without contrast enhancement
- endometriomas and hemorrhagic corpus luteal cysts are less likely to have a high T1 rim and do not usually involve the entire ovary
- T2: can have low signal due to interstitial hemorrhage
Treatment and prognosis
Urgent surgery is required to prevent ovarian necrosis. Most ovaries are not salvageable, in which case a salpingo-oophorectomy is required. If not removed, the necrotic ovary can become infected and cause an abscess or peritonitis. In the case of a non-infarcted adnexa, surgical untwisting can be performed. Mortality resulting from ovarian torsion is rare. Spontaneous detorsion has also been reported.
Differential diagnosis
For an enlarged edematous ovary +/- Fallopian tube, consider:
- pelvic inflammatory disease (PID): has a very different clinical presentation
- massive ovarian edema (MOO)
- oophoritis
Practical points
- the ovary should be tender to transducer pressure
- absence of ovarian Doppler flow is highly specific for torsion, but normal Doppler flow does not completely rule out torsion
- an ovarian mass causing the torsion must always be sought
Siehe auch:
- eingeblutete Ovarialzyste
- Dermoidzyste
- Endometriose
- Unterleibsentzündung
- Tubentorsion
- Ovarialtorsion bei Brenner-Tumor
- Paraovarialzysten
- Ovarialtorsion in der Schwangerschaft
- Zystadenom des Ovars mit Torsion
- Ovarialtorsion bei Ovarialfibrom
- massive ovarian oedema (MOO)
und weiter:


 Assoziationen und Differentialdiagnosen zu Ovarialtorsion:
Assoziationen und Differentialdiagnosen zu Ovarialtorsion: