Chondromyxoidfibrom











Chondromyxoid fibromas (CMFs) are extremely rare, benign cartilaginous neoplasms that account for <1% of all bone tumors .
Epidemiology
As with all rare lesions, reported epidemiology varies:
- age:
- most commonly diagnosed before 30 years of age (~75%), mostly during second and third decades
- full reported range from 3 to 70 years of age
- gender:
- conflicting data
- some series show slight male predilection
Clinical presentation
Typically patients present with progressive pain, often long-standing and/or bony swelling and restricted range of movement in affected limb . The latter is most often the case in bones with little overlying soft tissues (e.g. short tubular bones of the hands and feet).
Pathology
Microscopic examination, the tumor comprises of a variable combination of chondroid, myxoid, and fibrous tissue components organized in a pseudolobulated architecture . Additionally, occasional osteoclast-like giant multinucleated cells are encountered particularly at the periphery. Most cells are morphologically bland, and mitotic figures are rare or absent .
Macroscopic appearance
On gross examination, they are typically seen as solid glistening tan-gray intraosseous masses.
Location
Most chondromyxoid fibromas are located in the metaphyseal region of long bones (60%), and may extend to the epiphyseal line and even rarely abut the articular surface . They are almost never exclusively epiphyseal .
The classical site is the upper one-third of the tibia, which accounts for 25% of all cases, with the small tubular bones of the foot, the distal femur, and pelvis/sacrum being other relatively common locations .
Rare cases involving the calvarium/skull base , and mandible , as well as the sternum have been reported.
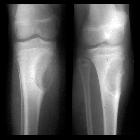
Radiographic features
Plain radiograph
- lobulated or oval eccentric lytic lesion
- well defined sclerotic margin: ~85%
- often expansile, with long axis parallel to long axis of long bone
- no periosteal reaction (unless a complicating fracture present)
- geographic bone destruction: almost 100%
- presence of septations (pseudotrabeculation): ~60%
- internal matrix calcification - uncommon by imaging (2-15%)
- perilesional sclerosis
MRI
MR features are often not particularly specific. Signal characteristics include:
- T1: low signal
- T1 C+ (Gd)
- majority (~70%) show peripheral nodular enhancement
- ~30% diffuse contrast enhancement and this can be either homogeneous or heterogeneous
- T2: intermediate to high signal
- areas of low signal, both in peripheral rim and centrally, may correspond to perilesional sclerosis and minimal internal mineralization, respectively
Nuclear medicine
On bone scans, the scintigraphic "doughnut sign" has been described in this tumor type . However, this is non-specific and can be seen in many other bone lesions.
Treatment and prognosis
They are benign lesions and malignant degeneration is rare. There is a high rate of reported recurrence (up to 80%) with curettage alone, with lower rate (~20%) with bone grafting. As such if an en-bloc resection is possible this is advisable .
History and etymology
It is thought to have been initially described by H L Jaffe and L Lichtenstein in 1948 .
Differential diagnosis
General imaging differential considerations include:
- aneurysmal bone cyst (ABC)
- giant cell tumor of bone (GCT)
- non-ossifying fibroma: younger age group
- chondroblastoma: younger age group
- metaphyseal fibrous defect
Siehe auch:
- Aneurysmatische Knochenzyste
- nicht ossifizierendes Fibrom
- Chondroblastom
- benigne Osteolysen
- Riesenzelltumor des Knochens
und weiter:
- endosteal scalloping
- Riesenzelltumor
- Knochentumoren
- Tumoren der Thoraxwand
- fibröser Kortikalisdefekt
- Ostitis fibrosa cystica
- differential diagnosis for metatarsal region pain
- lytic bone lesion (mnemonic)
- Osteoklastom
- myxoide Tumoren
- chondroide Tumoren
- Riesenzelltumor des Beckenknochens
- Knochenläsionen der Metaphyse
- Chondromyxoidfibrom der Tibia
- chondromyxoid fibroma of the calcaneus


 Assoziationen und Differentialdiagnosen zu Chondromyxoidfibrom:
Assoziationen und Differentialdiagnosen zu Chondromyxoidfibrom:



