DAI grading




Grading of diffuse axonal injury due to trauma is described according to the anatomic distribution of injury. Contrary to the implication of the word "diffuse," diffuse axonal injury has a topological predilection for focal involvement of certain sites in the brain. These sites, in turn, vary in functional importance.
Classification
Pathology
A classification based on histopathology was first proposed by J Hume Adams and colleagues in 1989 :
- grade 1: microscopic-only evidence of axonal damage in the white matter of the cerebral hemispheres including corpus callosum, in the brainstem, and, occasionally, in the cerebellum
- grade 2: focal lesion in the corpus callosum, in addition to diffuse axonal damage
- grade 3: focal lesions in both the corpus callosum and dorsolateral quadrant of the rostral brainstem, in addition to diffuse axonal damage
The features of diffuse axonal damage vary by time: axonal bulbs are present within days, microglia clusters and astrocytosis develop after weeks, and Wallerian degeneration of the white matter tracts sets in after months.
Focal lesions include infarct and hemorrhage. Focal lesions may sometimes be only identified microscopically. Grade 2 and 3 injury is considered severe if the focal lesions are macroscopically apparent.
MRI
Lindell Gentry translated the histopathologic grading system to imaging in the following manner in a review article in 1994 published in Radiology :
- stage 1 (lobar): diffuse axonal injury lesions confined to the lobar white matter, especially grey-white matter junction
- most common sites: parasagittal regions of frontal lobes, periventricular temporal lobes
- less common sites: parietal and occipital lobes, internal and external capsules, cerebellum
- stage 2 (callosal): diffuse axonal injury lesions in the corpus callosum, almost invariably in addition to the lobar white matter
- most common sites: posterior body and splenium of corpus callosum
- less common sites: anterior body and rostrum of corpus callosum (usually in conjunction with posterior involvement)
- usually unilateral and eccentric but may be bilateral and symmetric
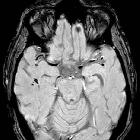
- stage 3 (brainstem): diffuse axonal injury lesions in the brainstem, almost invariably in addition to the lobar white matter and corpus callosum
- most common sites: dorsolateral midbrain, upper pons, and superior cerebellar peduncles
Diffuse axonal injury lesions were not clearly defined in this article by their MR appearance aside from being multiple, small, elliptical "lesions" located in characteristic areas of white matter. Small petechial hemorrhages, which appear hypointense on T2*-weighted images, are characteristic but represent a minority of true diffuse axonal injury lesions .
Prognosis
The prognostic validity of the MRI-based anatomic grading of diffuse axonal injury is controversial. Some point out that the Adams classification was inappropriately ported to MRI without robust study of its ability to predict outcome . Others have found supportive evidence for its prognostic utility: a meta-analysis including 5 studies of 258 patients with diffuse axonal injury found an unfavorable functional outcome in 17% of patients with grade 1 diffuse axonal injury on MRI, 40% of grade 2, and 63% of grade 3 . However, many smaller studies have found weak or nonexistent correlations between MRI grading and outcome, suggesting that clinical applicability in individual patients is likely poor . Some investigators have proposed alternative MRI location-based grading scales that may perform as well or better than the original Gentry classification, including those with added emphasis on the basal ganglia, thalamus, substantia nigra, and/or midbrain tegmentum .
It is unclear whether the variable sensitivity of different MRI techniques to detect diffuse axonal injury affects the predictive validity of anatomic grading (eg, SWI rather than T2* GRE, 3T rather than 1.5T) .
See also
- diffuse axonal injury (DAI)
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Diffuse axonal injury (DAI) grading:
Assoziationen und Differentialdiagnosen zu Diffuse axonal injury (DAI) grading: