gastrointestinale Vaskulitis

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. A practical flowchart for potential diagnostic work up of intestinal vasculitis following MRE or CTE

Imaging of
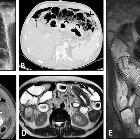
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal ischemia in a 37-year-old male with a history of known Henoch–Schönlein purpura (HSP) presenting with abdominal pain and bloody diarrhea. The patient underwent pre (A)- and post (B)-IV contrast CT scans using positive dilute oral contrast. Segmental mural thickening (thick white arrows) is seen in the terminal ileum with a focal area of mural hypoenhancement (thin white arrows) proximal to the ileocecal valve. Ileocolonoscopy confirmed mucosal ischemic changes, and signs/symptoms were improved following treatment by corticosteroid

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Crohn’s disease in a 23-year-old male presenting with abdominal pain and transient obstructive episodes. MRE was obtained. Axial T2-W image (A) shows multi-focal mural thickening in several segments of the ileum (thick white arrows) associated with increased mesenteric fat (white dotted ovals) separating the bowel loops. Coronal pre- and post-contrast T1-W images (B, C) demonstrate increased striated mural enhancement of the affected bowel segments (thin white arrows), more predominant on the mesenteric border. Engorgement of mesenteric vessels is depicted (white asterisks) representing comb sign. There is also pseudodiverticula formation along the antimesenteric border (white arrowheads)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Small bowel obstruction in a 31-year-old female with known scleroderma presenting with generalized abdominal pain, nausea, and vomiting without previous Hx of surgery. Axial view of CTE shows extensive cutaneous and subcutaneous calcifications (thick white arrows). Short segment benign-looking stricture (white arrowhead) is seen at the distal ileum in the pelvis, leading to upstream small bowel dilatation (white asterisks). Following segmental resection and anastomosis, this was confirmed to be a fibrotic stricture. Collapsed ileum distal to stricture is also depicted (thick black arrow)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Colonic pseudo-obstruction in a 35-year-old female with known scleroderma presenting with constipation, nausea, vomiting, and abdominal distension. CT scan with IV/oral contrast was done. Axial CT image (A) demonstrates dilation of the distal esophagus (thick white arrows), a common finding in scleroderma. Axial CT image (B) reveals marked diffuse dilatation of colon (*) without obvious wall thickening or abrupt transition point, suggestive for colonic pseudo-obstruction (Ogilvie syndrome)
Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and benign intestinal pneumatosis in a 52-year-old male with a history of known Scleroderma presenting with abdominal pain. Physical examination revealed generalized abdominal tenderness without rebound or guarding. Upright CXR (A) was done in the ER. Pneumoperitoneum (thick black arrows) was noted at CXR in the absence of signs or symptoms of peritonitis. Due to this discrepancy, abdominal CT scan (B, C) was performed and confirmed pneumoperitoneum (thin black arrow) along with extensive intestinal pneumatosis in the transverse colon (black arrowheads) and jejunum (thick white arrows). The patient underwent conservative treatment. He was discharged one week later with improved signs/symptoms. After three weeks, MRE was obtained and displayed no pneumoperitoneum. Axial T2-W image (D) demonstrates segmental jejunal mural thickening (white dotted oval) with hypointense appearance. Coronal T2-W image (E) shows bowel dilation and the classic hidebound sign (black dotted oval) in the ileum related to known scleroderma. The T2 hypointense segment of thick jejunum is also seen (curved arrows), suggestive of chronic mural thickening perhaps due to fibrosis

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Bowel stricture with secondary bacterial overgrowth in a 44-year-old male with a history of primary antiphospholipid antibody syndrome. He presented with abdominal pain, fever, nausea, vomiting, and diarrhea without a history of previous surgery. CTE was obtained. Axial CT (A) shows evidence of chronic SMV thrombosis associated with multiple collateral veins in the mesenteric root (white dotted oval). CT images (B–D) demonstrate diffuse mural thickening at jejunal loops with submucosal edema and mucosal hyperenhancement (thick white arrows). There is an abrupt stricture in a segment of proximal ileum (thin white arrows) leading to upstream bowel dilatation (white asterisks) suggestive of partial obstruction with development of ascites. The clinical and imaging findings were suspicious for focal stricture secondary to an old vascular insult with secondary bacterial overgrowth in dilated jejunal and proximal ileal loops. The patient underwent antibiotic therapy, bowel rest, and conservative management resulting in improvement of signs/symptoms. He was discharged with an uneventful follow-up

Imaging of
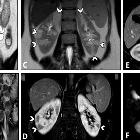
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and renal infarction in a 29-year-old female with known SLE presenting with fever, malaise, generalized abdominal pain, dyspnea, and elevated ESR. An abdominopelvic CT scan with IV and oral contrast was done. There are subpleural patchy areas of GGO at the left lower lobe suggestive of lupus pneumonitis (thick black arrows in A). Small pericardial effusion and thickening (thin white arrows in B) are seen in favor of serositis. There is a wedge-shaped subcapsular hypodensity in the spleen (white dotted oval in C), indicative of splenic infarction. Multiple bilateral wedge-shaped renal parenchymal infarcts are also depicted (thick white arrows in D). Diffuse circumferential wall thickening of ileal loops (white arrowheads in E and F) is evident, representing lupus enteritis

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 42-year-old female with a known history of SLE and hypothyroidism presenting with generalized abdominal pain, fever, anemia, and elevated inflammatory markers. She also complained of dysuria, hematuria, and frequency. MRE was obtained. Axial T2-W images (A, B) show bilateral hydroureteronephrosis (thin white arrows) and multi-focal segmental circumferential mural thickening involving several jejunal and ileal loops (thick white arrows). Axial T2-W image (C) displays an under distended urinary bladder containing a Foley catheter showing diffuse wall thickening (thick black arrows). Coronal T2-W and post-contrast T1-W images (D, E) demonstrate multi-segmental mural thickening involving several jejunal and ileal loops showing increased enhancement due to active nature of inflammation (black arrowheads). Submucosal edema is also noted (thin black arrow). Axial T2-W and post-contrast T1-W images (F, G) also reveal involvement of rectosigmoid colon (white dotted ovals). Small amount of free fluid is noted at the abdominopelvic cavity (black asterisks)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal ischemia in a 31-year-old female with known SLE-Sjögren overlap syndrome presenting with fever, anemia, and LUQ pain. MRE was obtained. Coronal T2-W and post-contrast T1-W images (A, B) display mural thickening, mucosal hypoenhancement, and serosal hyperenhancement of descending colon adjacent to the splenic flexure (thick white arrows) suggestive for mucosal ischemic changes. Coronal T2-W and post-contrast T1-W images (C, D) display mural thickening and increased mural enhancement of the cecum and ascending colon (Thin white arrows). Axial T2-W image and corresponding DWI sequence (E, F) show concentric mural thickening of the proximal ascending colon, demonstrating restricted diffusion (white arrowheads), in favor of ischemic changes or increased inflammatory cells. Coronal post-contrast T1-W image (G) reveals subcapsular areas of splenic hypoenhancement (white dotted oval), indicative of infarction. Pale and fragile mucosa is seen in colonoscopic view (H) of the involved colonic splenic flexure

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 26-year-old female with known Behçet’s disease and positive HLA-B5 complaining of episodic RLQ pain. MRE was obtained. Coronal T2-W image (A) demonstrates irregular circumferential mural thickening of the cecum and proximal ascending colon (thick black arrows) without mesenteric side predilection or pericolic infiltration. Coronal and axial post-contrast T1-W images (B, C) show marked enhancement of thickened colonic wall (thick white arrows) mildly extending to ileocecal valve (thin white arrow) with low-grade mural hyperenhancement in the adjacent terminal ileum (white arrowhead). Axial DWI image (D) obtained at a b-value of 800 s/mm2 reveals restricted diffusion in the thickened cecum (white dotted oval)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Terminal ileitis in a 23-year-old female with a history of recurrent oral and genital aphthous ulcers and uveitis presenting with RLQ pain finally diagnosed as Behçet’s disease. MRE was obtained. Coronal and axial T2-W images (A, B) show mural thickening in the terminal ileum (thick white arrows) without significant predilection to the mesenteric side in contrast to Crohn’s disease. There is also a deep penetrating ulcer (thin white arrow). Axial post-contrast T1-W image (C) displays increased contrast enhancement in the thickened terminal ileal segment (white arrowheads) without surrounding mesenteric inflammatory changes. Axial DWI image and corresponding ADC map obtained at b-value of 800 s/mm2 (D, E) show restricted diffusion in the involved segment (white dotted oval). Histopathologic examination confirmed Behçet’s disease

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and perforation in a 32-year-old male with a history of asthma presenting with abdominal pain and eosinophilia. MRE was obtained. Coronal and axial post-contrast T1-W images (A, B) display increased mural enhancement at the terminal ileum without thickening (thick white arrows). Three months later (C, D), the patient presents to the ER with acute abdominal pain without definite diagnosis or treatment. Chest X-ray (C) shows subdiaphragmatic free gas (thick black arrow). He underwent an emergency laparotomy. Intraoperative photograph (D) revealed focal bowel perforation at the distal ileal segment. After segmental bowel resection, an ileostomy was performed. Eight months after surgery (E, F), he was admitted for RUQ pain and dyspnea. Axial chest CT image (E) demonstrates bilateral GGO and consolidations with lobular distribution (white dotted oval). Axial contrast-enhanced CT image (F) shows multiple wedge-shaped areas of hypoattenuation in the liver (thin white arrows), consistent with hepatic infarction. Intraparenchymal gas formation is also evident at the infarcted segment, suggestive for abscess formation (black dotted oval). Small-vessel vasculitis was confirmed based on clinical/laboratory data and pathology results suggestive of Churg–Strauss syndrome. Unfortunately, he died secondary to sepsis

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. The diagnosis of intestinal vasculitis is based on a combination of the clinical manifestation and history, imaging, laboratory, and histopathology findings

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 28-year-old male with leukocytoclastic vasculitis presenting with abdominal pain, chest discomfort, and erythematous rashes with palpable purpura on the lower extremities. An abdominopelvic CT scan with IV and oral contrast was obtained. Axial images (A, B) show mild bilateral pleural effusion and pelvic free fluid. Also, axial CT (C) demonstrates mild concentric mural thickening of the distal ileal loop (thin black arrows). The patient underwent a biopsy of skin lesions. The histopathologic study revealed leukocytoclastic vasculitis. Corticosteroid therapy started. Then, MRE was done after five days. Axial post-contrast T1-W images (D, E) display mild mural thickening and hyperenhancement (thick white arrows) in the distal ileal segments. Mild engorgement of adjacent mesenteric vessels (white dotted oval) is also evident, and there is no ascites. Imaging findings and clinical data were indicative of an excellent response to therapy

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and pulmonary alveolar hemorrhage in a 41-year-old male with ANCA-positive granulomatosis with polyangiitis (GPA) presenting with abdominal pain and hemoptysis. Axial thoracic CT images (A, B) at two different levels show diffuse mosaic attenuation secondary to geographic areas of ground-glass opacity, suggestive for alveolar hemorrhage. Follow-up CT images (C, D) three days after corticosteroid therapy demonstrate a notable response to treatment. CTE was also done with suboptimal small bowel distention (E, F) at admission to assess the cause of abdominal pain that revealed circumferential mural thickening at ascending colon and distal ileum (thin white arrows) associated with adjacent mesenteric fat haziness. Follow-up CT images (G, H) show complete response to corticosteroid therapy with normal bowel wall thickness (thick white arrows) and a decrease in attenuation of the ileocolic mesenteric root
Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 39-year-old female presenting with episodic abdominal pain and findings of non-specific terminal ileitis in ileocolonoscopy examination. MRE was obtained. Coronal T2-W and post-contrast T1-W images (A, B) display mild mural thickening and hyperenhancement at distal terminal ileum (thick white arrows). Coronal T2-W and post-contrast T1-W images (C, D) reveal multiple peripheral wedge-shaped hyperintense areas at both kidneys, showing decreased enhancement on delayed phase (white arrowheads). Axial post-contrast T1-W and corresponding DWI images (E, F) show a hypoenhancing lesion at the right renal cortex with diffusion restriction (thin white arrows). Vasculitis was suspected as the underlying cause. Afterward, positive results for antineutrophil cytoplasmic antibody (ANCA) and inflammatory markers were consistent with the diagnosis of ANCA-associated vasculitis

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and perforation in a 56-year-old male with known ANCA-positive granulomatosis with polyangiitis and long history of immunosuppressive therapy presenting with acute abdominal pain and leukocytosis. Chest X-ray (A) shows two pulmonary nodules projecting over the lower zone of the left hemithorax (black dotted ovals). MRE was obtained. Axial T2-W image (B) reveals multi-focal segmental mural thickening in jejunal loops (thin black arrows). Axial post-contrast T1-W image (C) displays intense mural hyperenhancement (thin white arrows) in the involved segments. Focal intestinal pneumatosis (white dotted ovals) is also evident. Axial T2-W image (D) shows pneumoperitoneum (white arrowheads) at the non-dependent portion of the abdominal cavity, indicating bowel perforation. Coronal T2-W image (E) demonstrates small amount of free fluid (thick white arrows) at the abdominal cavity. Due to acute nature of presentation, the patient subsequently underwent laparotomy. Intraoperative photograph (F) reveals focal bowel necrosis and perforation. No signs of peritonitis were found in the initial examination, more likely due to the immunocompromised status of the patient

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Vasculitis of splanchnic arteries in a 43-year-old male with a history of pathologically proven polyarteritis nodosa and segmental jejunal resection due to ischemia. He complains of postprandial abdominal pain, nausea, vomiting, hypertension, and elevated inflammatory markers. CTE was done. Axial and sagittal images (A–C) in the arterial phase demonstrate severe stenosis at the origin of the celiac trunk (thin white arrows) and complete occlusion and irregularity of proximal SMA (thin black arrows). Coronal CT images (D–F) reveal vessel irregularity and mild degree of aneurysmal dilations in a collateral branch between celiac trunk and SMA (white arrowheads), thickening and irregularity in jejunal branches of SMA (black dotted oval) adjacent to the previous site of jejunal resection and anastomosis (white curved arrows). The ileocolic branch of SMA also shows focal aneurysmal dilatation and mild thickening (white dotted oval)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 32-year-old female with PAN (polyarteritis nodosa) presenting with episodic abdominal pain, fever, anemia, and elevated liver enzymes and inflammatory markers. MRE was obtained. Coronal and axial T2-W images (A, B) show a single thickened segment of mid ileum (thick white arrows) with mild T2 hyperintensity more likely secondary to submucosal edema. This is associated with mild degree of upstream bowel distention. Coronal and axial post-contrast T1-W images (C, D) display mural hyperenhancement (thin white arrows) with a relatively striated pattern. DWI at a b-value of 800 s/mm2 (E) shows restricted diffusion (white arrowhead), suggesting increased inflammatory cell density. The patient underwent double-balloon enteroscopy following this MRE, but it was complicated by bowel perforation at this segment. Then, surgical resection and ileostomy were performed. Histopathological assessment of resected segment revealed vasculitis consistent with polyarteritis nodosa (PAN). Heterogeneous enhancement of liver at arterial phase is also depicted (C), which raises suspicion for microvascular involvement (white dotted oval)

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis in a 35-year-old female with known Takayasu arteritis presenting with RLQ pain and elevated ESR. Axial contrast-enhanced CT scan (A) shows mural thickening and severe stenosis at the origin of the celiac artery (thin black arrow). Axial CT image (B) demonstrates circumferential mural thickening and submucosal edema at a single distal ileal segment (elbow arrow). MRE (C) was done following corticosteroid therapy after six days. Axial T2-W image shows complete resolution of corresponding ileal involvement (thick white arrow). Axial post-contrast T1-W image (D) displays concentric and irregular mural thickening and enhancement of abdominal aorta (black dotted oval) with double rings appearance (inner low and outer high enhancement). MR angiography (E) was performed. MIP image shows irregularity and multi-segmental stenosis at the distal abdominal aorta (thin white arrows). There is also bilateral stenosis at the origin of renal arteries (white arrowheads). The proximal segment of SMA shows irregularity and severe stenosis (white dotted oval). Abnormal dilatation of the arc of Riolan (white curved arrows) is evident, which supplies collateral flow to the SMA territory

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Schematic illustration on the spectrum of vasculitis related damage on the vessel wall

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Diagram of various types of vasculitis based on the size of the affected vessel and etiology

Gastrointestinal
perforation: clinical and MDCT clues for identification of aetiology. 75-year-old patient with vasculitis. a Coronal contrast-enhanced illustrates pneumatosis intestinalis, and poor enhancement of the horizontal and ascending duodenum (arrowheads) and adjacent fat stranding. Note an incidental diverticulum (d) at the 2nd part of the duodenum, moderate amount of free fluid (f) and gas bubbles (open arrows) at the porta hepatis. b Axial CT image demonstrates gas in the superior mesenteric vein (black arrow) with adjacent fat stranding

Gastrointestinal
manifestations of Systemic Lupus Erythematosus: What needs to be considered in an acute setting?. Fig-1: (a)Topogram of abdomen showing thumb-printing (arrow) suggestive of ischemic colitis; (b) Axial sections plain & post contrast showing rectus sheath hematoma (star); (c)target appearance (white arrow) of ascending colon with intramural haemorrhage.

Imaging of
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Segmental arterial mediolysis (SAM) in a 55-year-old male presenting with epigastric pain for ten days and normal laboratory results. Axial, sagittal, and coronal images from CTE (A–D) show fusiform aneurysmal dilatation of two jejunal branches of SMA associated with partial mural thrombosis (thick white arrows). Coronal CTE (E) demonstrates aneurysmal dilation and high-grade thrombosis at a jejunal branch of SMA (white arrowhead) with sparing of proximal arterial bifurcation (white dotted oval)
gastrointestinale Vaskulitis
Vaskulitis Radiopaedia • CC-by-nc-sa 3.0 • de
Vasculitis describes generalized inflammation of vessels. Vasculitides carry a broad range of clinical presentations and as a whole can involve almost any organ system.
Pathology
Some vasculitides are due to direct vessel injury from an infectious agent. However a large proportion show evidence of immune complex related vessel wall injury.
Classification
There are many, often overlapping, types of classification:
- Lie classification of vasculitis (1994)
- 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides
Siehe auch:
- Polyarteriitis nodosa
- Rheumatoide Arthritis
- Churg-Strauss-Syndrom
- Granulomatose mit Polyangiitis
- Vaskulitis
- Morbus Behçet
- Takayasu-Arteriitis
- Riesenzellarteriitis
- Kawasaki-Syndrom
- Mikroskopische Polyangiitis
- Dünndarmbeteiligung bei Purpura Schönlein-Henoch
- IgA-Vaskulitis
- gastrointestinale Vaskulitis bei systemischem Lupus Erythematodes
- Cogan-Syndrom
- cryptoglobulinemic vasculitis
- Vaskulitis der Gallenblase
- leukozytoklastische Vaskulitis


 Assoziationen und Differentialdiagnosen zu gastrointestinale Vaskulitis:
Assoziationen und Differentialdiagnosen zu gastrointestinale Vaskulitis:










