lateral epicondylitis












Lateral epicondylitis, also known as tennis elbow, is an overuse syndrome of the common extensor tendon and predominantly affects the extensor carpi radialis brevis (ECRB) tendon.
Epidemiology
Lateral epicondylitis occurs with a frequency seven to ten times that of medial epicondylitis. As with medial epicondylitis, it typically occurs in the 4 to 5 decades of life. There is no recognized gender predilection.
Clinical presentation
Patients often present with lateral elbow pain, tenderness and swelling, which is frequently exacerbated when they grasp objects during wrist extension with resistance. A history of tennis playing or similar racket sports is sometimes elicited, but the condition often results from other repetitive athletic or occupational activities, or without an identifiable cause.
Pathology
It is thought that repetitive stress and overuse leads to tendinosis involving the origin of the extensor tendons at the lateral elbow, with microtearing and progressive degeneration due to an immature reparative response that may progress to a full-thickness tendon tear. Alternatively, it may also result from direct trauma.
Histology demonstrates tendinosis, enthesopathy, disorganization of collagen architecture, mucoid change, fibrosis and variable vascular proliferation.
Radiographic features
MR imaging is the most widely used modality, although ultrasound may also be performed.
Plain radiograph
Up to 25% of patients with lateral epicondylitis may have calcification within the soft tissue around the lateral epicondyle, representing calcific tendinopathy or enthesopathy.
Ultrasound
Thickening of the common extensor tendon, associated with diffuse heterogeneity and areas of focal hypoechogenicity. There is often associated intra-tendon calcification and bony irregularity at the tendon insertion. The most common finding in a patient with lateral epicondylitis is focal areas of hypoechogenicity with a background of intrinsic tendinopathy. Color Doppler may show tendon hyperemia. Dynamic assessment can also be performed to delineate instability.
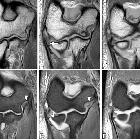
MRI
The hallmarks of tendinosis and tearing of the common extensor tendon on MRI are abnormal morphology and signal intensity, as follows :
- the best clue for the diagnosis of lateral epicondylitis is an abnormal thickening and increased signal intensity within the common extensor origin from the lateral epicondyle
- abnormal thickening and abnormal separation of the radial collateral ligaments and the ECRB tendon with granulation tissue
- the imaging findings of tendinosis must be correlated with clinical data of lateral epicondylitis because if the patient is asymptomatic in the presence of these findings, the case may be attributed to subclinical diagnosis or early tendon degeneration
- partial or even full-thickness tear of the ECRB tendon complicating tendinosis may be encountered in patients with lateral epicondylitis; it is manifested as fluid-filled gap with or without loss of fiber continuity; tears can sometimes be graded as low, intermediate and high grade depending upon the thickness of tear i.e <20%, 20-80% and >80% respectively
- peritendon edema and associated focal bone marrow edema at the site of tendon attachment to the humerus may simulate avulsion injury
- in chronic cases, increased signal intensity of the nearby anconeus muscle may be seen
- associated radial nerve entrapment may occur in 5% of cases
- the radial collateral ligament may also be disrupted
Treatment and prognosis
Initially, conservative treatment and rehabilitation should be attempted which include cessation of the offending activity, applications of ice, administration of nonsteroidal anti-inflammatory drugs or corticosteroid injection, and use of a splint or brace.
Autologous blood injection has been shown to more effective at long-term relief than corticosteroid injection, with 90% of patients in one study being pain-free at six months . Whole blood injection has been shown to be just as an effective as platelet-rich plasma injection and is also much less expensive .
Surgical intervention is reserved for the recalcitrant cases if 6 to 9 months of conservative treatment failed. However, in professional athletes, it may be only after 3-6 months.
History and etymology
It was initially described by Henry Morris as “lawn tennis arm” in 1882 and now most commonly termed as tennis elbow.
Differential diagnosis
For a clinical differential diagnosis of lateral elbow pain, consider:
- occult fracture
- osteochondritis dissecans of the capitellum
- lateral osteoarthrosis
- lateral ulnar collateral ligament (LUCL) instability
- radial tunnel syndrome
Siehe auch:
- Osteochondrosis dissecans
- Ellenbogen
- Epicondylitis ulnaris humeri
- radial tunnel syndrome
- Ruptur des gemeinsamen Ursprung der Extensoren am Ellenbogen
- Epicondylitis
und weiter:


 Assoziationen und Differentialdiagnosen zu Tennisellenbogen:
Assoziationen und Differentialdiagnosen zu Tennisellenbogen: