neuroendokrine Dünndarmtumoren

Neuroendokriner
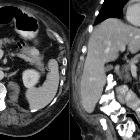
Tumor des Ileums mit mesenterialer Lymphknotenmetastase in der Computertomographie: Oben Primarius der Ileumschlinge im wesentlichen nach intraluminal wachsend, jedoch auch mit organüberschreitender Infiltration. Unten Lymphknotenmetastase des Mesenteriums mit typischer desmoplastischer, sternförmige Reaktion. Verkalkungen in der Metastase. Die beiden linken Bilder jeweils in arterieller Phase, die anderen portalvenös. Der Patient war durch Subileusbeschwerden auffällig geworden.

Neuroendokriner
Tumor des terminalen Ileums mit mesenterialer Lymphknotenmetastase und mesenterialer desmoplastischer Reaktion.
neuroendokrine Dünndarmtumoren
gastrointestinale neuroendokrine Tumoren Radiopaedia • CC-by-nc-sa 3.0 • de
Gastrointestinal neuroendocrine tumors (GI NETs) can be functional or non-functional:
- functional NETs can be challenging to localize as:
- they are often small in size at the time of diagnosis
- arise in many sites throughout the body
- non-functioning and/or malignant NETs often are larger at presentation and therefore easier to locate
Pathology
Types of gastrointestinal - pancreatic neuroendocrine tumors
- insulinoma
- account for 50% of pancreatic NETs
- usually <2 cm diameter
- 99% of insulinomas found in pancreas
- 10-15% are malignant
- gastrinoma
- account for 20-30% of pancreatic NETs
- found in pancreas, lymph nodes and duodenum
- vary in size
- 60-75% are malignant
- non-functioning tumors and pancreatic polypeptide secreting tumors
- account for 15-20%
- almost exclusively found in pancreas
- usually malignant
- often large at presentation
- vasoactive polypeptide secreting tumor (VIPoma)
- account for 3%
- 90% found in the pancreas
- 10% found in adrenal gland
- 50-60% are malignant
- glucagonomas and somatostatinomas
- rare
- most commonly located in pancreas
- often malignant
Radiographic features
There is no consensus on the best single imaging modality for NETs and it depends on the suspected location and local expertise. Combined modalities and techniques are often used :
CT
- used for suspected gastric, enteric and pancreatic NETs pre and post IV iodinated contrast
- bowel distension with fluid, either by oral intake (CT enterography) or via a nasojejunal tube (CT enteroclysis) improves detection of primary GI NETs
MRI
Used for suspected hepatic, pancreatic or retroperitoneal NETs, often with gadolinium contrast agents. MRI enterography also possible.
Ultrasound
- used for monitoring slow growing tumors and/or follow up of metastases.
- ultrasound can also be used to guide biopsies.
- endoscopic/endoluminal US can be used to identify and characterize GI NETs as well as obtaining samples for cytology and/or histology
Nuclear medicine
- common radiopharmaceutical is In-pentetreotide, which is a ligand for the somatostatin receptor on the cell membrane of many NETs
- multiple tumor sites and/or metastasis can be identified using a gamma-camera to detect the emitted radiation
- can be used in combination with cross-sectional imaging modalities to aid staging e.g. SPECT, PET/CT or PET/MRI
- can be used to predict response to nuclear medicine based therapies, and, in some cases, to assess response to treatment.
- care should be taken with interpretation of images as drugs can interfere with somatostatin receptor expression, e.g. interferon
- NETs can differentiate into tumors that do not express somatostatin receptors, becoming ‘imaging-occult’ making recurrence or metastases more challenging to detect
- other radiopharmaceuticals are also used, based on certain physiological characteristics e.g. cell surface receptors or uptake of molecules.
- gallium-68 labeled somatostatin analogs (PET/CT) – thought to be more sensitive in detecting NETs except pulmonary and hepatic metastases
- for aggressive, rapidly growing tumors (i.e. high metabolism) fluorodeoxyglucose-PET/CT can be used (FDG-PET)
- F-DOPA and C-hydroxytryptophan may be used in future but are not routinely available
Angiography
- venous sampling can be used in small functional NETs where cross-sectional imaging is equivocal
- multiple endocrine neoplasia type 1 can present with multiple lesions; functional NETs can be identified from these, using calcium stimulation with venous sampling
- angiography and endovascular procedures, such as transarterial chemo-embolization (TACE), can be used to treat hepatic metastases
Practical points
Assessing specific gastrointestinal NET imaging based on location
- gastric or colonic - endoscopy
- small bowel
- contrast enhanced CT/MR enterography, +/- radiopharmaceuticals or gallium PET/CT to localize NETs as classically high concentration of somatostatin receptors and are very vascular
- capsule endoscopy may be helpful to detect small bowel NETs not identified by CT or MRI but precise location can be difficult
- pancreatic NETs
- non-functioning NETs present late and tend to be larger and have mass-effect or non-specific symptoms or signs; these can be identified using CT
- functioning NETs present early with signs and symptoms, leading to clinical suspicion of tumor which is often smaller and more challenging to locate
- triple phase thin multislice CT (pre-contrast/arterial/portal venous)
- high resolution MRI with T2, T1, fat saturated and dynamic contrast administration
- PET/CT or PET/MRI
Assessing primary malignancy
Signs on CT of malignant NETs include
- larger size
- necrosis
- calcification
- invasion of the surrounding structures
Assessing staging and metastases
- commonly metastasizes to lymph nodes and the liver, as well as bone, lung, and mesentery
- 40-80% of midgut NETs present with metastases at presentation
- Union for International Cancer Control (UICC) TNM (tumor, node, metastasis) systems or the European Neuroendocrine Tumor Society (ENETS) have TNM staging systems which differ slightly from each other
See also
Siehe auch:
- Neuroendokriner Tumor
- Dünndarmkarzinoid
- De-Grouchy-Syndrom Typ 2
- gastrointestinale neuroendokrine Tumoren
und weiter:


 Assoziationen und Differentialdiagnosen zu neuroendokrine Dünndarmtumoren:
Assoziationen und Differentialdiagnosen zu neuroendokrine Dünndarmtumoren: