Patellar maltracking







Patellofemoral instability is the clinical syndrome due to morphologic abnormalities in the patellofemoral joint where the patella is prone to recurrent lateral dislocation.
Epidemiology
Most patients with patellar instability are young and active individuals, especially females in the second decade. Prevalence is 6-77 per 100,000 population .
Pathology
The normal patellofemoral joint has two kinds of stabilizers - active stabilizers (extensor muscles) and passive stabilizers (bones and ligaments):
- bone stabilizers: deep femoral sulcus, high lateral trochlea
- ligament stabilizers: medial patellofemoral retinaculum, medial patellofemoral ligament
Three major morphologic abnormalities which predispose to patellar instability:
- trochlear dysplasia: trochlear joint surface is flattened
- patella alta
- lateralization of the tibial tuberosity: femorotibial malrotation, genu recurvatum
Other factors contributing to patellar instability are
- increased femoral anteversion
- ligament or retinaculum injury or laxity (Ehlers-Danlos syndrome, Marfan syndrome)
- abnormal muscle tone
The most common mechanism of first-time patellar dislocation is internal rotation of the femur relative to the knee (i.e. exorotation of the tibia relative to the femur) while the foot is planted and the knee is flexed.
Radiographic features
Plain radiograph
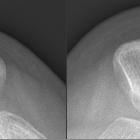
The "crossing sign" represents abnormally elevated floor of the trochlear groove rising above the top of the wall of one of the femoral condyles, assessed on lateral radiographs. "Double contour sign" is a double line at the anterior aspect of condyles, and seen if medial condyle is hypoplastic. Skyline view can show decreased trochlear depth and large sulcus angle (>144º).
MRI
Lateral trochlear inclination, trochlear facet asymmetry, and trochlear depth are used to judge trochlear dysplasia.
Classification of trochlear dysplasia (Dejour et al)
- type A: normal shape of the trochlea, but a shallow trochlear groove
- type B: markedly flattened or even convex trochlea
- type C: trochlear facet asymmetry, with too high lateral facet, and hypoplastic medial facet
- type D: type C features and a vertical link between facets ('cliff pattern')
Lateral trochlear inclination
The most superior section showing trochlear cartilage is selected for this measurement. The inclination is the angle formed between the plane of the lateral trochlear facet subchondral bone and a tangential line through posterior femoral condyles. An angle of <11º is considered abnormal.
Trochlear facet asymmetry
This is the ratio of medial trochlear facet width to lateral trochlear facet width and measured in the axial plane. A ratio of <0.4 is considered abnormal (i.e. it is abnormal if the medial facet is <40% the width of the lateral facet).
Trochlear depth
This measures the inset depth of the trochlear groove (sulcus) relative to the mean of the medial and lateral femoral condyle outsets. It is determined by axial imaging at the same level as the trochlear facet asymmetry. A trochlear depth of <3 mm is considered abnormal.
Patella alta
Patella alta (or a high riding patella) describes a situation where the position of the patella is considered high. See patella alta article for a description of the Insall-Salvati ratio.
Patellar translation
Patellar translation, known as the TT-TG distance (tibial tubercle to trochlear groove distance) is currently advocated as an accurate measure of patellar instability. The distance from the tibial tuberosity to the trochlear groove is measured parallel to the tangential line through posterior femoral condyles:
- <15 mm is considered normal
- 15-20 mm is considered borderline
- >20 mm is considered abnormal
The distance has been shown to be slightly less when measured on MRI than CT .
Associated radiological features of patellar instability
- knee joint effusion
- medial patellofemoral ligament tear
- bone contusion in the patella and lateral condyle
- osteochondral defects in the patella
- edema/hemorrhage of vastus medialis
- intra-articular loose bodies
- internal derangement of the knee
Treatment and prognosis
Nearly half of the patients with first-time dislocation will sustain recurrent dislocation after conservative management. Chronic patellar instability, if not treated, may lead to severe arthritis and chondromalacia patellae. The aim of the surgery is to repair the knee damage caused by patellar dislocation and to correct the primary anatomical anomaly. Surgical modalities are:
- medial patellofemoral ligament reconstruction
- trochleoplasty
- medialisation of the tibial tuberosity
- medial capsular plication
Siehe auch:
- Chondromalacia patellae
- Patella alta
- Marfan-Syndrom
- femoropatellare Dysplasie
- mediales Retinaculum patellae
- Double contour sign
- crossing sign of trochlear dysplasia
- crossing sign
- double contour sign of trochlear dysplasia
- Ligamentum patellofemorale mediale
- patellar subluxation
- Ligamentum patellomenisceale (MPML)
und weiter:


 Assoziationen und Differentialdiagnosen zu femoropatellare Instabilität:
Assoziationen und Differentialdiagnosen zu femoropatellare Instabilität: