pelvines Kongestionssyndrom
















Pelvic congestion syndrome (some prefer pelvic venous insufficiency ) is a condition that results from retrograde flow through incompetent valves in ovarian veins. It is a commonly missed and potentially-treatable cause of chronic abdominopelvic pain.
Epidemiology
It tends to be more common in multiparous, premenopausal women who typically present with chronic pelvic pain for more than 6 months . The overall population prevalence may approach ~10%.
Clinical presentation
Patients often have non-cyclical chronic (typically dull and aching) pelvic pain. In certain cases there may be thigh or vulvar varices. It is often considered a diagnosis of exclusion.
Pathology
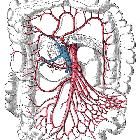
Pelvic congestion syndrome is considered the female equivalent to a testicular varicocele. It is caused by:
- venous obstruction: such as retroaortic left renal vein
- compression of left renal vein by SMA also known as nutcracker phenomenon
- incompetent valves in ovarian vein
Radiographic features
The diagnosis of pelvic congestion syndrome is established by the demonstration of multiple dilated, tortuous parauterine veins with a width >4 mm or an ovarian vein diameter greater than 5-6 mm .
Ultrasound
- ovarian vein >5-6 mm (positive predictive value of 71-83%)
- may show multiple dilated veins in the adnexa with reversed venous flow on color Doppler, especially after Valsalva maneuver
- the venous calibers may increase on real time during Valsalva
- prominent myometrial veins may also be present
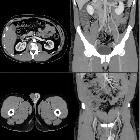
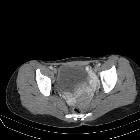
CT
Contrast enhanced CT typically shows dilated pelvic and ovarian veins. The supine position during scanning may underestimate the size of venous dilatation.
MRI
MR venography
May show dilated veins. Time of flight (TOF) imaging can be performed where contrast is not required.
Signal characteristics
- T1: seen as flow voids which represent engorged arcuate vessels
- T2: mostly high signal but can vary dependent on velocities from low signal to iso signal
- GE: high signal
Treatment and prognosis
Treatment options include coil embolization of the gonadal vein: ovarian vein embolization. Surgical (e.g. laparoscopic) ligation of the ovarian vein may also be an option in selected cases. The presence of multiple collaterals between iliac and ovarian venous plexuses may cause recurrence of symptoms.
History and etymology
Pelvic congestion syndrome was first described in 1857 by Louis Alfred Richet (1816-1891), a French anatomist and surgeon .
See also
Siehe auch:
- Arteria mesenterica superior
- Varikozele
- Nussknacker-Syndrom
- Ovarialvenenthrombose
- Phlebolithen in Ovarialvene
- Varicocele der Vena ovarica
- Vena ovarica
- varikös erweiterte periuterine Venen
- Embolisation Vena ovarica
- akuter Beckenschmerz
- ovarian vein embolisation
- periprostatische Varizen
- spontane Ruptur der Vena ovarica
- Varizen der Labien
und weiter:


 Assoziationen und Differentialdiagnosen zu pelvines Kongestionssyndrom:
Assoziationen und Differentialdiagnosen zu pelvines Kongestionssyndrom: