placenta previa





Placenta previa refers to an abnormally low lying placenta such that it lies close to, or covers the internal cervical os. It is a common cause of antepartum hemorrhage.
Placenta previa is a potentially life-threatening condition for both mother and infant. As such, antenatal diagnosis is essential to adequately prepare for childbirth.
Epidemiology
Placenta previa has an incidence of 1/200 pregnancies.
Risk factors
Placenta previa is associated with a number of risk factors, including:
- previous placenta previa
- previous cesarean section
- increased maternal age
- increased parity
- large placentas
- multiple gestations
- erythroblastosis
- maternal history of smoking
- assisted conception
- previous manual removal of placenta
Associations
- abnormal placental villous adherence (~5%): e.g. placenta accreta
Clinical presentation
Placenta previa usually presents with painless vaginal bleeding in the second half of pregnancy (>20 weeks gestation), most commonly between 34-38 weeks gestation.
Other associated clinical features include:
- high fetal presenting part
- maternal/fetal compromise secondary to exsanguination
Pathology
The term "placenta previa" covers a spectrum of anomalies and results from the partial or total insertion of the placenta into the lower uterine segment.
Classification
Previa is divided into four grades depending on the relationship and distance to the internal cervical os:
- grade I: low-lying placenta: placenta lies in the lower uterine segment but its lower edge does not abut the internal cervical os (i.e lower edge 0.5-2.0 cm from internal os).
- grade II: marginal previa: placental tissue reaches the margin of the internal cervical os, but does not cover it
- grade III: partial previa: placenta partially covers the internal cervical os
- grade IV: complete previa: placenta completely covers the internal cervical os
Sometimes grades I and II are termed a "minor" or "partial" placenta previa, and grades III and IV are termed a "major" placenta previa .
Radiographic features
Ultrasound
Due to placental trophotropism, the diagnosis of a placenta previa is not usually made before 20 weeks.
During the 'routine' 18 to 21-week morphology scan, the distance between the lower edge of the placenta and the internal os should be measured. If it lies within a few centimeters of the cervical os, then a repeat ultrasound at ~32 weeks should be performed to ensure that the edge has migrated further away.
MRI
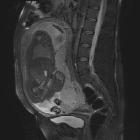
MRI is the gold standard imaging modality for the placenta and its relationship to the cervix, although in most instances it is not required. Sagittal images best demonstrate the relationship of the placenta to the internal cervical os.
Treatment and prognosis
A low-lying placenta is relatively common in the second-trimester morphology scan. As the fetus grows and the uterus expands, the lower uterine segment thins and grows disproportionately, such that in most cases the placenta is no longer low-lying by a follow-up study (usually performed at 32-34 weeks).
In the case of a complete placenta previa, a cesarian section is required for delivery to avoid the risk of fetal and maternal hemorrhage.
History and etymology
Previa is of Latin origin. It is a combination of 'prae' (meaning before) and 'via' (meaning way).
Differential diagnosis
- full bladder
- focal myometrial contraction
These can make the placenta appear closer to the internal cervical os than it actually is (particularly on a second trimester scan). Postvoid images should always be obtained if previa is suspected.
Occasionally, a subchorionic hematoma that extends over the cervix can mimic placenta previa, especially if the hemorrhage is still echogenic. Follow-up imaging would be useful to distinguish the two entities.
Practical points
- transvaginal ultrasound scan is more accurate to assess placenta previa, the transabdominal scan may overdiagnose it in up to one-quarter of cases
- when spotted in the second trimester, a third-trimester ultrasound scan (~32-34 weeks) should be performed to reassess the placenta position
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Placenta praevia:
Assoziationen und Differentialdiagnosen zu Placenta praevia: