Pneumothorax (ultrasound)





Pneumothorax is a serious potential consequence of blunt thoracic trauma and, if misdiagnosed, it may quickly become life-threatening.
For a discussion on epidemiology, clinical presentation, pathology, and treatment and prognosis please see the main pneumothorax article.
Radiographic features
CT is considered the gold-standard in the diagnosis of pneumothorax. Thoracic ultrasound has more sensitivity than a supine chest radiograph (see: supine pneumothorax) for the identification of pneumothorax after blunt trauma. The other advantage of ultrasound is that it can be used at point-of-care.
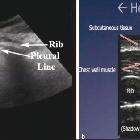
The normal lung interface with pleura shows lung sliding with z-lines, which appear as vertical comet tails running down from the pleural surface. In pneumothorax, this sliding is absent and so are the comet tail artifacts from the pleura. The sight of even a single B-line excludes pneumothorax at that location. There is also loss of the lung pulse, the subtle lung oscillation in tandem with cardiac contraction, which is especially important when trying to distinguish between right mainstem intubation (loss of sliding on the left, but lung pulse is present) and a left sided pneumothorax (no sliding or lung pulse). Free intrathoracic air will then reflect incident ultrasound waves, obscuring the visceral pleura beneath; while all dynamic signs will be abolished, A-lines will be seen extending into the far field.
Visualizing the junction between sliding lung and absent sliding is known as the lung point sign and is near 100% specific for pneumothorax. One may use the mid-axillary line as a landmark for subsequent semi-quantification of the pneumothorax volume. It is not able to be found in all pneumothoraces (sensitivity is around 65%) especially large pneumothoraces where the lung is collapsed and there is globally absent sliding.
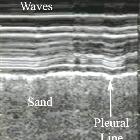
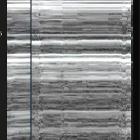
On M mode, classical signs for the gray scale imaging are seen:
- seashore sign: normal lung sliding
- barcode/stratosphere sign: pneumothorax
History and etymology
The use of ultrasound to diagnose pneumothorax was first described in a veterinary medical journal in 1986 .
Differential Diagnosis
The bilateral, anterior discovery of sliding lung is sufficient to rule out pneumothorax in the vast majority of cases. Bilateral absence of B-lines/comet tail artifacts from the pleura with loss of the lung pulse and sliding, and subsequent discovery of a lung point in a typical location is quite specific for the presence of a pneumothorax. The differential for bilaterally absent lung sliding includes:
- fibrotic lung disease
- abdominal compartment syndrome
- status asthmaticus
- apnea
- cardiopulmonary arrest
Unilateral loss of sliding may suggest :
- right mainstem bronchus intubation, in the context of chest trauma and recent endotracheal intubation
- a vigorous lung pulse will be present, as the visceral and parietal pleura are still apposed
- ultrasound may be used, real-time, to "guide" the endotracheal tube proximally, confirming position with the bilateral return of lung sliding and diaphragmatic excursion
- complete atelectasis
- early signs of atelectasis are dynamic; sliding is lost, there is no lung point to be found, the lung pulse is unmasked, the diaphragm is elevated with reduced excursion
- a posterolateral tissue-like pattern develops over time, with the early presence of static air bronchograms, often lost as the air is resorbed
- if loss of sliding and an A-line pattern meet a perpendicular, anechoic collection, the hydro-point is defined
- pathognomonic for a fluid-air interface e.g. a hydropneumothorax
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Pneumothoraxdiagnostik mittels Sonographie:
Assoziationen und Differentialdiagnosen zu Pneumothoraxdiagnostik mittels Sonographie: