Posterolateral rotatory instability of the elbow










Posterolateral rotatory instability of the elbow is the most common pattern of elbow instability, most commonly seen following posterior elbow dislocation . It is characterized by :
- posterolateral subluxation/dislocation of the radial head relative to capitellum
- posterior displacement of ulna relative to the trochlea
- intact proximal radioulnar joint
Posterolateral rotatory elbow instability indicates injury to the stabilizing structures of the posterolateral elbow, particularly the lateral collateral ligament complex.
Clinical presentation
Patients may present with vague lateral elbow pain, popping, snapping and/or clicking. These symptoms may, in particular, brought up by activities which place the elbow in its unstable position of external rotation of the forearm with valgus and axial loading, such as pushing up from a chair or doing push-ups.
Most patients can recall a traumatic event, frank elbow dislocation or fall in outstretched hands.
Active and passive provocative tests can be helpful to make a diagnosis. Specific tests include lateral pivot shift, lateral pivot-shift apprehension test, posterolateral rotatory drawer test, chair sign, or active floor push-up sign.
Pathology
The normal elbow is laterally stabilized by :
- radial collateral ligament complex
- lateral ulnar collateral ligament (LUCL) considered the primary contributor to lateral elbow stability
- radiocapitellar articulation
- coronoid process
- common extensor origin (lesser contribution)
Damage to the medial (ulnar) collateral ligament complex, together with one more supporting structures, may result in posterolateral rotational elbow instability during elbow extension and forearm supination. The pattern consists of posterolateral subluxation or dislocation of the radial head relative to capitellum, as well as posterior displacement of ulna relative to the trochlea.
A common mechanism of injury is from fall on an outstretched hand with the forearm in supination, causing a pattern of soft tissue injury which progresses from lateral to medial. Thus, the lateral collateral ligament complex is first injured, followed by anterior/posterior capsule, and eventually, the medial collateral ligament which would result in a full elbow dislocation. The proximal radioulnar joint typically remains intact, and so the forearm bones externally rotate as a unit relative to the humerus.
Etiology
- trauma: most common
- chronic attenuation of lateral ulnar collateral ligament: due to chronic microtrauma or chronic cubitus varus from a prior distal humeral fracture
- iatrogenic: from steroid injection or lateral epicondylitis procedures with the inadequate repair of the lateral ulnar collateral ligament, or radial head resection
Radiographic features
Plain radiograph
Normal or the “drop sign” may be seen, which is the posterior subluxation of the radial head compared to capitellum on a lateral x-ray.
Osborne-Cotterill lesion represents a shear or depression fracture of the capitellum and the lateral condyle and/or an avulsed fragment attached to the lateral ulnar collateral ligament. This usually accompanies contusion or fracture of the radial head, mostly in the anterior aspect.
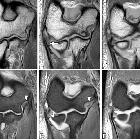
MRI
Conventional MRI or MR arthrogram may be helpful to demonstrate lateral ulnar collateral and other ligament injuries.
Treatment and prognosis
Management of the elbow instability varies according to patient symptoms.
Non-operative management, including avoidance of provocative maneuvers, elbow bracing, and pain control may be attempted in mild cases or where surgery is contraindicated.
Symptomatic posterolateral rotatory elbow instability is commonly managed by surgical reconstruction of the ulnar collateral ligament complex. Direct repair of an otherwise healthy ligament, or else autologous or allograft (e.g. palmaris longus tendon) reconstruction may be performed by open or arthroscopic approach . Additional corrective measures may include radial head or coronoid reconstruction to correct the bone deficiency, and humerus osteotomy to correct varus deformity across the elbow joint .
If there is no established osteoarthritis of elbow joint at the time of surgery, outcomes may be good to excellent .
Siehe auch:
- Osborne-Cotterill-Läsion
- Ligamentum anulare radii
- Ellenbogeninstabilität
- Ruptur Ligamentum anulare radii
und weiter:


 Assoziationen und Differentialdiagnosen zu posterolaterale Rotationsinstabilität des Ellenbogens:
Assoziationen und Differentialdiagnosen zu posterolaterale Rotationsinstabilität des Ellenbogens:

