Ellenbogeninstabilität




















Elbow instability refers to as an excessive, usually painful, mobility in the elbow joint, most of the time as a result of a prior traumatic event or overuse and maybe also seen in patients with connective tissue disease .
Classification
Elbow instability can be classified in respect of timing (acute, chronic, recurrent), part of joint involved (ulnohumeral, radiocapitellar, proximal radioulnar), degree and direction of displacement and the coexistence of associated fractures :
- posterolateral rotatory instability (most common)
- valgus instability (posttraumatic / repetitive microtrauma)
- varus instability (elbow dislocations)
- posteromedial rotatory instability
- anterior instability (rare)
Clinical presentation
Patients usually complain of a characteristic history of either a fall in acute instability or recurrent pain with snapping, popping, locking, clicking or clunking in chronic instability and/or the direct complain and apprehension of subluxation .
Clinical testing includes assessing the physiological range of motion in the elbow joint, where noticeable problems might already occur as well as clinical tests as the lateral pivot-shift test, posterolateral drawer test and posterolateral rotatory apprehension test, table-top relocation test, gravity-assisted varus stress test, etc. .
Pathology
Usually involves acute, chronic or repetitive osseous and /or soft tissue injury of the following structures :
- primary static elbow stabilizers/restraints :
- ulnohumeral joint
- medial (ulnar) collateral ligament complex, in particular, the anterior bundle (AMCL)
- lateral (radial) collateral ligament complex, in particular, the lateral ulnar collateral ligament (LUCL)
- secondary static elbow stabilizers/restraints:
- radiocapitellar joint
- common flexor origin
- common extensor origin
- joint capsule
- dynamic stabilizers/restraints
Etiology
Acute instability, dislocations and subluxations usually result from a fall on the outstretched hand (FOOSH) or other acute traumatic event and the eccentric loading forces which act upon the elbow joint and its stabilizing structures .
Chronic and recurrent instability occurs as a result of previous posttraumatic injuries or repetitive microtrauma e.g. repetitive valgus stress in baseball pitching .
Radiographic features
Plain radiograph
Dislocations, subluxations, misalignment and associated (avulsion-) fractures or other underlying osseous abnormalities and may be seen in routine elbow radiographs .
Increased ulnohumeral distance (≥4mm) on a lateral radiograph following reduction is referred to as “drop sign” and indicates instability.
Stress radiographs may show radial head subluxation or ulnohumeral joint asymmetry
CT
Can characterize bony structures in fracture-dislocations or depict subtle fractures e.g. in posteromedial rotatory instability .
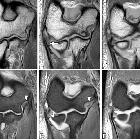
MRI
The main utility of MRI lies in the detection of the underlying ligamentous and soft tissue injuries, especially the medial (ulnar) collateral ligament complex in case of valgus instability and to characterize the extent of ligamentous and muscular injury in posterolateral rotatory instability .
Treatment and prognosis
Depending on the instability pattern the age of the patient and other comorbidities treatment varies.
Acute elbow dislocations, not complicated by fractures are treated with closed reduction and subsequent brief immobilization .
Associated fractures should be treated with open reduction, if the elbow is unstable, especially olecranon fractures, which involve the anterior joint surface and the insertion of the ligaments and radial head fractures as well as coronoid process type II and type III fractures .
Posterolateral rotatory elbow instability is usually managed surgically especially in young patients and athletes .
Older patients with associated comorbidities and osteoarthritis may be managed conservatively.
Siehe auch:
- Ellenbogenluxation
- Osborne-Cotterill-Läsion
- Verletzungen des lateralen Kollateralbandes am Ellenbogen
- medial collateral ligament injury elbow
- posterolaterale Rotationsinstabilität des Ellenbogens
und weiter:


 Assoziationen und Differentialdiagnosen zu Ellenbogeninstabilität:
Assoziationen und Differentialdiagnosen zu Ellenbogeninstabilität:
