Primary pneumatosis intestinalis

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Pneumoperitoneum (green arrow) and air dissecting the fat abdominal planes (yellow asterisk) were incidental findings in this chest X-ray performed for the depiction of a PICC (orange arrow).

Bening
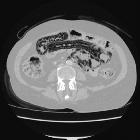
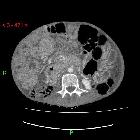
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show pneumatosis intestinalis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show pneumatosis intestinalis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show pneumatosis intestinalis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show pneumatosis intestinalis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show pneumatosis intestinalis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Bening
pneumatosis intestinalis with worrisome radiological findings at first glance. Axial (a,b,c,d), coronal (d) and sagittal (e) CT images on pulmonary window show intestinal pneumatosis (blue arrows), air dissecting the fat abdominal planes (yellow asterisk) and pneumoperitoneum (green asterisk).

Pneumatosis
Intestinalis in HIV and MAC co-infection. On lung windows, the intramural gas seen on the abdominal radiograph was much more conspicuous.
Pneumatosis
Intestinalis in HIV and MAC co-infection. Small bowel wall thickening and gross ascities.

Pneumatosis
Intestinalis in HIV and MAC co-infection. Admission abdominal radiograph shows gross pneumatosis intestinalis of the large bowel. When compared with an earlier abdominal film three months ago, similar but less severe pneumatosis was demonstrated.

Pneumatosis
Intestinalis in HIV and MAC co-infection. Abdominal radiograph three months prior demonstrates less severe pneumatosis.

Pneumatosis
intestinalis versus pseudo-pneumatosis: review of CT findings and differentiation. Pneumoperitoneum in a 66-year-old man with a history of scleroderma and multiple episodes of pneumatosis intestinalis spontaneously resolved in 24 h. a Axial unenhanced CT at a lung window shows pneumoperitoneum (arrow). b Axial unenhanced CT shows oesophageal dilation (arrow), indicating patulous oesophagus associated with scleroderma
Imaging of
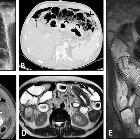
intestinal vasculitis focusing on MR and CT enterography: a two-way street between radiologic findings and clinical data. Intestinal vasculitis and benign intestinal pneumatosis in a 52-year-old male with a history of known Scleroderma presenting with abdominal pain. Physical examination revealed generalized abdominal tenderness without rebound or guarding. Upright CXR (A) was done in the ER. Pneumoperitoneum (thick black arrows) was noted at CXR in the absence of signs or symptoms of peritonitis. Due to this discrepancy, abdominal CT scan (B, C) was performed and confirmed pneumoperitoneum (thin black arrow) along with extensive intestinal pneumatosis in the transverse colon (black arrowheads) and jejunum (thick white arrows). The patient underwent conservative treatment. He was discharged one week later with improved signs/symptoms. After three weeks, MRE was obtained and displayed no pneumoperitoneum. Axial T2-W image (D) demonstrates segmental jejunal mural thickening (white dotted oval) with hypointense appearance. Coronal T2-W image (E) shows bowel dilation and the classic hidebound sign (black dotted oval) in the ileum related to known scleroderma. The T2 hypointense segment of thick jejunum is also seen (curved arrows), suggestive of chronic mural thickening perhaps due to fibrosis
Primary pneumatosis intestinalis (PPI) is a benign idiopathic condition in which multiple gas-filled cystic lesions are seen in the gastrointestinal tract wall. The changes are usually seen initially on radiography or CT with CT being the more sensitive test.
Epidemiology
Primary pneumatosis intestinalis is rare and was shown in one study to comprise 15% of cases of all intestinal pneumatosis .
Clinical presentation
This condition is usually asymptomatic and presents as an incidental finding on medical imaging.
Pathology
Multiple gas-filled cysts are seen in the mucosa and submucosa of the small and large bowel.
Differential diagnosis
- ischemic bowel: gas in the ischemic bowel wall has a linear or bubble-like pattern, in contrast to the PPI gas pattern, which is circular
- causes of secondary pneumatosis intestinalis
- post-instrumentation of the bowel e.g. endoscopy, surgery
- COPD, ventilated patients
- drugs such as steroids, chemotherapy (e.g. bevacizumab)
- pseudopneumatosis: intraluminal gas trapped between feces and the bowel wall
See also
Siehe auch:
- Pneumatosis intestinalis
- Unterscheidung Pseudo-Pneumatosis intestinalis - echte Pneumatosis intestinalis
- pneumatosis intestinalis (mnemonic)
- Pneumatosis intestinalis bei Sklerodermie
- Pneumatosis intestinalis bei Methotrexat
- chronische Pneumatosis intestinalis bei HIV
- Pneumatosis intestinalis bei COPD
und weiter:


 Assoziationen und Differentialdiagnosen zu benigne Pneumatosis intestinalis:
Assoziationen und Differentialdiagnosen zu benigne Pneumatosis intestinalis:

Unterscheidung
Pseudo-Pneumatosis intestinalis - echte Pneumatosis intestinalis