Pneumatosis intestinalis
































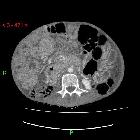





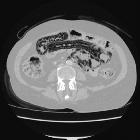


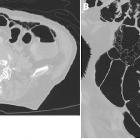
Intramural bowel gas, also known as pneumatosis intestinalis, refers to the clinical or radiological finding of gas within the wall of the bowel.
Terminology
There are different terminologies in the medical literature, such as pneumatosis intestinalis, pneumatosis coli, and pneumatosis cystoides intestinalis. Pneumatosis coli is used when only the colic wall is involved and is generally an incidental finding in asymptomatic patients. Pneumatosis cystoides intestinalis is descriptive for multiple gaseous cysts along the bowel wall.
Pathology
Intramural gas can be seen in intestinal ischemia and eventually bowel infarction. This is the most concerning etiology for intramural gas.
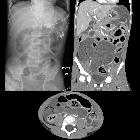
Gas in the bowel wall in the neonatal period, whatever its shape, is diagnostic of necrotizing enterocolitis.
Asymptomatic pneumatosis intestinalis may result from a variety of interrelated contributing factors including:
- mucosal integrity
- intraluminal pressure
- bacterial flora
- intraluminal gas
Due to disruption in mucosal integrity with increased mucosal permeability, gas forming bacteria can enter the submucosa and can produce predominantly hydrogen gas. Another theory is mechanical pressure from pulmonary diseases like COPD leads to pneumatosis intestinalis.
Benign pneumatosis can be caused by a variety of reasons such as pulmonary disease, systemic disease (scleroderma, lupus, AIDS), intestinal inflammation, iatrogenic/procedures, medications (steroids, chemotherapeutic drugs, Lactulose, sorbitol and voglibose), and organ transplation.
Life-threatening pneumatosis can be caused by intestinal ischemia, obstruction, enteritis/colitis, toxic caustic ingestion, toxic megacolon, organ transplantation, and collagen vascular disease.
Radiographic features
Gas tracks along the bowel wall, appearing as either linear, which are usually submucosal, or rounded cystic "bubbly" collections, which are usually subserosal . Where they join, they may outline the circumferenial margin of the bowel, creating rings (this circular pattern of PI favors a benign pathology, whereas the linear and bubbly lucencies can be associated with any i.e either benign or life threatening causes) .
Gas in the bowel wall is most easily identified with CT and plain radiography, but ultrasound and MRI can be usefully in pediatric patients where there is a desire to avoid radiation.
A common diagnostic dilemma is differentiate benign pneumatosis from clinically worrisome causes . The following are imaging features of clinically worrisome pneumatosis:
- soft tissue bowel wall thickening
- free intraperitoneal fluid
- lesser extent of pneumatosis (more extensive pneumatosis is more commonly benign)
- periintestinal soft-tissue stranding
- abnormal bowel wall enhancement
- atherosclerosis and vascular occlusion
The presence of pneumomediastinum favors a benign cause . Pneumoperitoneum and pneumoretroperitoneum can be seen with both idiopathic and ischemic pneumatosis
Differential diagnosis
- bowel ischemia and infarction
- infection
- inflammatory bowel disease
- medication-induced
- chemotherapy
- steroid use
- autoimmune disease and immunosuppression
- connective tissue disorders
- primary pneumatosis
- pulmonary disease
- idiopathic
- iatrogenic
- post endoscopy / colonoscopy
- post operative
- post enteric tube
- CT colonography
- pseudopneumatosis (mimics) include:
- gas trapped between bowel wall and luminal contents
- gas trapped by opposing mucosal folds
- gas bubbles adherent to bowel wall
Practical points
From a clinical perspective, it is essential not to confuse the incidental imaging finding of asymptomatic pneumatosis with symptomatic colonic perforation because the treatment is significantly different .
See also
- a helpful mnemonic for remembering the causes of pneumatosis intestinalis
- abnormal intra-abdominal gas
- necrotizing enterocolitis (NEC)
- pneumatosis cystoides intestinalis
- pneumatosis coli
Siehe auch:
- Koprostase
- Mesenterialinfarkt
- Nekrotisierende Enterokolitis
- portalvenöses Gas
- Pneumatosis coli
- emphysematöse Zystitis
- Unterscheidung Pseudo-Pneumatosis intestinalis - echte Pneumatosis intestinalis
- Divertikulose
- abnormales Gas im Abdomen
- pneumatosis intestinalis (mnemonic)
- Pneumatosis cystoides des Kolons
- Ischämiezeichen Darm
- benigne Pneumatosis intestinalis
- Pneumatosis intestinalis bei Sklerodermie
- Pneumatosis intestinalis bei immunsupprimierten Patienten
- Gas in der Ösophaguswand
- emphysematöse Kolitis
- Pneumatosis intestinalis bei Methotrexat
- cystic intestinal pneumatosis
- Pneumatosis cystoides intestinalis (PCI)
und weiter:


 Assoziationen und Differentialdiagnosen zu Pneumatosis intestinalis:
Assoziationen und Differentialdiagnosen zu Pneumatosis intestinalis: