prostatic carcinoma



































Prostate cancer ranks as the most common primary malignant tumor in men and the second most common cause of cancer-related deaths in men. Prostatic adenocarcinoma is by far the most common histological type and is the primary focus of this article.
Epidemiology
It is primarily a disease of the elderly male. In the United States, approximately 200,000 new cases are diagnosed each year.
Clinical presentation
Prostate cancer is usually detected by:
- an elevated (greater than 4 ng/dL) prostate-specific antigen (PSA); normal is 1-4 ng/dL
- abnormal digital rectal examination
- the prostate gland is divided into several anatomic zones and prostate cancer usually arises within the peripheral zone near the rectum, which is why a digital rectal exam (DRE) is a useful screening test
Clinically patients can present with:
- urinary symptoms, e.g. nocturia, hesitancy, urgency, terminal dribble
- often collectively known as LUTS (lower urinary tract symptoms)
- hematuria (in advanced disease)
- back pain (from metastatic spread to the spine)
Clinical scores that may be useful in assessing symptoms severity include:
- IPSS: international prostate symptoms score, 35 points score mainly assessing urinary symptoms
- IIEF: international index of erectile function
Pathology
95% of prostate cancers are adenocarcinomas which develop from the acini of the prostatic ducts . They arise in the posterior/peripheral (70%) prostate gland more commonly than in the anterior gland and central zone (30%) .
Prostate cancer can spread by local invasion (typically into the bladder and seminal vesicles; urethral and rectal involvement are rare), lymphatic spread (pelvic nodes first followed by para-aortic and inguinal nodes), or by haematogenous metastases . Common sites of haematogenous metastases are :
- bone (90%)
- lung (~45%)
- liver (~25%)
- pleura (~20%)
- adrenal glands (~15%)
Histology
Pathologic specimens are graded using the Gleason score, which is the sum of the most prevalent and second most prevalent types of dysplasia, each on a scale of 1 to 5, with 5 being the most dysplastic.
Staging
TNM staging system is used for staging prostate cancer. Prostate cancer is one of the (less common) causes of cannonball metastases to the lung.
Radiographic features
Ultrasound
Transrectal ultrasonography (TRUS) is often initially performed to detect abnormalities and to guide biopsy, usually following an abnormal PSA level or DRE.
Ultrasound is used to direct biopsy of suspicious, hypoechoic regions, usually in the peripheral zone. Because of the high incidence of multifocality, systematic sextant biopsies are recommended.
On ultrasound, prostate cancer is usually seen as a hypoechoic lesion (60-70%) in the peripheral zone of the gland but can be hyperechoic or isoechoic (30-40% of lesions).
Transrectal ultrasound is also the modality of choice for directing brachytherapy seeds into the prostate gland.
MRI
The primary indication for MRI of the prostate is in the evaluation of prostate cancer after an ultrasound-guided prostate biopsy has confirmed cancer in order to determine if there is extracapsular extension . Increasingly MRI is also being used to detect and localize cancer when the PSA is persistently elevated, but routine TRUS biopsy is negative. Both the American College of Radiology (ACR) and European Society of Uroradiology (ESUR) advocate the use of multiparametric MRI (mpMRI) in prostate imaging .
MRI-guided prostate biopsy is also being used, particularly in those cases where TRUS biopsy is negative but clinical and PSA suspicion remains high . Following radical prostatectomy, patients with elevated PSA should also be examined using MRI.
Often a PI-RADS score is given to assess the probability of the lesion being malignant.
Signal characteristics
- T1: useful for detection of prostate contour, neurovascular bundle encasement, and post-biopsy hemorrhage
- T2
- using an endorectal coil, on T2-weighted images prostate cancer usually appears as a region of low signal within a normally high signal peripheral zone
- most significant cancers occur along the posterior portion of the prostate gland abutting the rectum
- DWI/ADC: often shows restricted diffusion
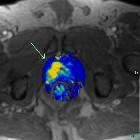
- dynamic contrast enhancement (DCE): (dynamic contrast enhancement in prostate cancer)
- shows enhancement but it can be difficult to distinguish from prostatitis or benign prostatic hyperplasia (especially in the central zone lesions )
- more specific than T2 signal
- involves post-processing time
- MR spectroscopy: (MR-spectroscopy in prostate cancer)
- increased choline: citrate or choline+creatine: citrate ratios are seen in prostate cancer (see below for more details)
Routine use of body 3.0 T magnets now means that endorectal coils have become unnecessary for prostate imaging due to the improved signal to noise and spatial resolution associated with higher field strength.
MRI parameters routinely assessed include the presence of a mass with a low T2 signal, restricted diffusion with reduced ADC, and increased tissue capillary permeability using dynamic contrast-enhanced (DCE) imaging and calculation of the so-called K (a calculated time constant for permeability). These so-called multiparametric techniques are increasingly being used in the assessment of prostate malignancy with MRI .
Extracapsular extension carries a poor prognosis. Assess for:
- asymmetry/extension into the neurovascular bundles
- obliteration of the rectoprostatic angle
- involvement of the urethra
- seminal vesicle invasion (normal seminal vesicles have high signal on T2)
Lymphadenopathy is best appreciated on T1-weighted images.
MR spectroscopy
The addition of MR spectroscopy (MRS) with fast T2-weighted imaging is an area of research that holds promise for the detection of disease. The normal prostate produces a large amount of citrate from the peripheral zone, which tumors do not . In normal prostate tissue citrate and polyamine levels are high and choline levels low. The reverse is the case in a tumor.
CT
Not accurate at detecting in situ prostate cancer. Scans of the abdomen and pelvis are commonly obtained before the onset of radiation therapy to identify bony landmarks for planning.
In advanced disease, a CT scan is the test of choice to detect enlarged pelvic and retroperitoneal lymph nodes, hydronephrosis, and osteoblastic metastases .
Nuclear medicine
Tc-99m MDP bone scan
- technetium-99m bone scan is usually used to detect osseous metastases
Ga-68-PSMA PET
- gallium-68-PSMA PET can be used for diagnosis, staging, restaging, evaluation of therapy response and prognostication in prostate cancer
F-18-fluciclovine PET
- fluorine-18-fluciclovine PET is used to detect and localize suspected prostate cancer recurrence based on elevated prostate-specific antigen in men who have undergone prior treatment
Treatment and prognosis
Generally, patients with a Gleason score of <7 and a PSA of <10 ng/L are considered to have potentially curable disease. These patients undergo prostatectomy, brachytherapy, or external beam radiation .
Patients that do not meet these criteria will usually undergo a combination of hormone therapy and external beam radiation.
Differential diagnosis
General imaging differential considerations include:
- benign prostatic hypertrophy (BPH)
- prostatic sarcoma
- rhabdomyosarcoma of the prostate: different demographics , i.e. much younger age group
- leiomyosarcoma of the prostate
- other prostatic tumors: rare (e.g. melanoma of prostate )
- direct invasion of the prostate by bladder or rectal adenocarcinoma
Differential considerations (mimics) on MRI include :
- anterior fibromuscular stroma: anterior, symmetric, usually hypointense
- central zone of the prostate: symmetric, central, tends not to wash out on DCE
- periprostatic veins and periprostatic lymph nodes
- bacterial prostatitis
- granulomatous prostatitis
- amyloidosis (rare)
- calcification, necrosis, hemorrhage


 Assoziationen und Differentialdiagnosen zu Adenokarzinom der Prostata:
Assoziationen und Differentialdiagnosen zu Adenokarzinom der Prostata: 


