radiologically isolated syndrome
Radiologically isolated syndrome (RIS) is defined by MRI findings meeting the McDonald criteria for multiple sclerosis in the brain and/or spinal cord in asymptomatic patients. Radiological progression usually occurs in approximately 66% of patients with RIS, while ~33% per 5-year-period will subsequently develop neurological symptoms that allow a definite diagnosis of multiple sclerosis .
Terminology
The incidental detection of brain and/or spinal cord lesions compatible with multiple sclerosis in MRI studies performed for other indications than demyelinating disorders is referred to as radiologically isolated syndrome (RIS) .
Development of neurological symptoms in patients with RIS is called conversion.
While the phenomenon of an asymptomatic, subclinical or clinically silent disease state of multiple sclerosis, incidentally discovered on autopsy and later imaging studies, has long been known, the extensive availability of MRI has led to a significant number of studies performed for indications other than inflammatory demyelinating disorders of the CNS, giving rise to this syndrome.
Epidemiology
While the exact prevalence is unknown owing to its incidental nature, RIS is the most common type of asymptomatic multiple sclerosis . One large retrospective cohort study stated prevalence as low as 0.05% or as high as 0.1-0.7% depending on methodology and definitions. Prevalence might be higher in relatives to patients suffering from multiple sclerosis .
Clinical presentation
Patients with RIS must not have neurological dysfunction suggestive of multiple sclerosis based on history and physical examination . Extreme caution should be applied to applying the diagnostic criteria in patients with chronic headache .
Radiographic features
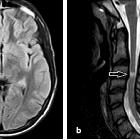
The criteria for RIS is defined by the McDonald criteria for dissemination in space, with or without dissemination in time, in asymptomatic patients. The imaging factors that predict conversion to multiple sclerosis include contrast-enhancing lesions, higher T2 lesion load, presence of infratentorial lesions, and spinal cord lesions ; of these, spinal cord lesions are the best predictor .
Treatment and prognosis
As stated above, radiological progression has been shown to occur in ~66% of patients with RIS. While the conversion rate roughly equates to 33% per 5-year-period, a significant number of patients will not subsequently develop multiple sclerosis.
Due to the absence of clear risk factors defining clinical conversion and lack of current evidence usually, no treatment is usually initiated.
Differential diagnosis
In older patients, especially those with vascular risk factors, chronic small vessel disease is an alternative consideration. A higher number of periventricular lesions should be considered before settling on the diagnosis of RIS.
In younger patients, migraine should be considered. These white matter lesions are small/punctate, rarely infratentorial, and nonprogressive. A perivenular distribution and intralesional signal loss would be more suggestive of RIS/MS .
Siehe auch:
- mikroangiopathische Leukenzephalopathie
- Encephalomyelitis disseminata
- McDonald Diagnostic Criteria for MS
- clinically isolated syndrome (CIS)
- MAGNIMS consensus on MRI diagnosis of multiple sclerosis
und weiter:


 Assoziationen und Differentialdiagnosen zu radiologically isolated syndrome:
Assoziationen und Differentialdiagnosen zu radiologically isolated syndrome: