solitärer fibröser Tumor
















Solitary fibrous tumors are a rare neoplasm of mesenchymal origin that comprise less than 2% of all soft tissue tumors. The majority are benign, although up to 20% may be malignant.
For a discussion of specific presentations of SFT, please refer to:
- solitary fibrous tumor of the pleura
- solitary fibrous tumor of the spinal cord
- solitary fibrous tumor of the dura
Epidemiology
Intrathoracic SFT usually presents in the 6 to 7 decades. Extrathoracic SFT occurs in men and women of all ages equally .
Clinical presentation
Although typically asymptomatic, it may present with symptoms and signs related to extrinsic compression of adjacent organs. Rarely solitary fibrous tumors result in non-islet cell tumor hypoglycemia (NICTH) as a result of secretion of insulin-like growth factor-2 (IGF-2) . Rarer still is acromegaly .
Pathology
Location
The majority of solitary fibrous tumors occur in an intrathoracic location but up to one third may occur in extrathoracic locations, and as such, they may be encountered essentially anywhere, including :
- pleura
- spinal cord
- dura
- head and neck
- extremities
- abdominal parenchymal organs
- retroperitoneum
- peritoneum
- pelvic organs
Histology
SFT most likely arises from submesothelial fibroblasts and used to be included in hemangiopericytoma spectrum .
At histology, a collagenous matrix with arrays of spindle cells is usually seen. Areas of necrosis, cystic or myxoid change, calcification, hemorrhage, increased vascularity, atypia, or malignancy may also be seen .
Immunohistochemistry
Immunohistochemical analysis can play an important role in the diagnosis and management :
- ~75% of benign solitary fibrous tumors of the thorax stain for CD34, a marker for normal endothelium and vascular tumors
- B-cell lymphoma 2 protein (Bcl-2), a marker of terminal differentiation, and vimentin are also positive in the majority of benign solitary fibrous tumors
- cytokeratin, S-100, and p53 proteins have shown increased expression in malignant solitary fibrous tumors
Radiographic features
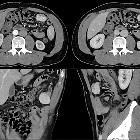
CT
CT reveals a well-circumscribed, smooth, and lobulated soft tissue mass that may contain scattered calcifications. Smaller tumors tend to enhance homogeneously, whereas larger lesions may have central tubular or rounded low-attenuation areas due to cystic or necrotic change.
MRI
On MRI, benign solitary fibrous tumors usually have relatively homogeneous low-to-intermediate signal intensity relative to skeletal muscle on both T1-weighted imaging and T2-weighted imaging because of fibrous tissue, as well as intense enhancement.
In addition, there may be areas of subacute hemorrhage that have high T1-weighted signal intensity, as well as non-enhancing cystic or necrotic foci that are more heterogeneous and higher in T2-weighted signal intensity relative to the remainder of the tumor.
However, when a central focus of heterogeneity and variable contrast enhancement is identified in an SFT at CT or MRI, malignant degeneration should be considered .
Treatment and prognosis
- benign SFT <10 cm in size typically has a favorable outcome with surgical resection alone
- SFT >10 cm that also harbors malignant foci, and has positive surgical margins tend to have a poor prognosis despite surgical treatment
- optimal adjuvant therapy for this group is unknown, and close-interval follow-up is advised because there is an increased incidence of local recurrence
Siehe auch:
- solitärer fibröser Tumor der Pleura
- Hämangioperizytom
- solitärer fibröser Tumor der Dura
- solitärer fibröser Tumor des Rückenmarks
- solitärer fibröser Tumor der Leber
- maligner solitärer fibröser Tumor der Pleura
- solitärer fibröser Tumor des Retroperitoneums
- solitary fibrous tumour in the paranasal sinuses
- maligner solitärer fibröser Tumor
- solitärer fibröser Tumor der Niere
- solitärer fibröser Tumor der Harnblase
- solitärer fibröser Tumor des Peritoneums
und weiter:


 Assoziationen und Differentialdiagnosen zu solitärer fibröser Tumor:
Assoziationen und Differentialdiagnosen zu solitärer fibröser Tumor:





