spinal synovial cyst














Spinal synovial cysts are cystic formations connected to the facet joint and containing synovial fluid lined by a cuboid or pseudostratified columnar epithelium. They may result in lumbar radiculopathy in a significant number of cases.
Clinical presentation
They may be asymptomatic and found incidentally. However, larger cysts can result in stenosis of the spinal canal and cause compression of neural structures resulting in associated clinical symptoms.
Pathology
Uncomplicated cysts are internally lined with cuboid or pseudostratified columnar epithelium and filled with clear or straw-colored fluid.
Associations
They are typically associated with adjacent facet joint arthropathy.
Location
- synovial cysts in the spine occur predominantly in the lumbar region as compared to thoracic and cervical regions
- in the lumbar spine, there may be a predilection towards the L4-5 level
Radiographic features
CT
Typically seen as a calcified cystic lesion adjacent to a facet joint . CT may also show adjacent facet joint arthropathy +/- the presence of gas.
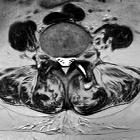
MRI
This entity cannot be reliably distinguished from ganglion cyst on standard MRI. However, communication with the joint space after intra-articular injection with contrast reliably differentiates the two.
- gas within the cyst is pathognomonic for a synovial cyst
- facet joint cysts may contain complex fluid as a result of internal debris or hemorrhage
- neural-based cysts can usually be differentiated by imaging as these cysts show intimate relation with the adjacent nerve, rather than with the adjacent joint space
Calcification within cyst wall appears low signal intensity on both T1 and T2 weighted images whereas hemorrhagic cysts display increase intensity compared to CSF likely due to T1 shortening from methemoglobin.
The cysts do not always possess the signal characteristics of a simple cyst, so contrast administration may be needed in some cases. It is important to remember that they are a cause of peripherally enhancing masses in the extrathecal space anywhere along the spinal canal.
Treatment and prognosis
Cysts can be operated upon or accessed percutaneously.
Percutaneous approach
The patient is positioned prone, followed by CT guided access into the inferior articular recess using a spinal needle. Once an intra-articular location is confirmed with contrast, and communication with the synovial cyst is demonstrated, rupture of the cyst is attempted using a steroid and anesthetic mixture.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Synovialzysten der Facettengelenke:
Assoziationen und Differentialdiagnosen zu Synovialzysten der Facettengelenke: