stress fracture

















































 nicht verwechseln mit: pathologische Fraktur
nicht verwechseln mit: pathologische FrakturStress fractures refer to fractures occurring in the bone due to a mismatch of bone strength and chronic mechanical stress placed upon the bone.
Terminology
A pathological fracture, although a type of insufficiency fracture, is a term in general reserved for fractures occurring at the site of a focal bony abnormality. Some authors use the term stress fracture synonymously with fatigue fracture, and thus some caution with the term is suggested.
Epidemiology
Fatigue fractures are common in athletes, especially runners and military recruits. Insufficiency fractures occur more in women and older people .
Risk factors
The following conditions increase the risk of a stress injury :
- female sex
- low bone density
- nutritional disorders or deficiencies
- 'female athlete triad'
- long-distance running
- inappropriately short recovery time
- training changes
- inadequate shoes
Clinical presentation
Stress fractures normally present with worsening pain with a history of minimal or no trauma. In the lower (weight-bearing) limb, there is often a history of a recent increase of physical activity or significant alteration in the type or duration of normal athletic activity.
Pathology
A stress fracture is the final stage of a stress injury and occurs if the bone fails to withstand a repetitive, cumulative loading force and is no longer capable to mitigate that loading stress with its own healing capabilities and breaks .
Etiology
- fatigue fracture: abnormal stresses on normal bone
- insufficiency fracture: normal stresses on abnormal bone
Location
Stress fractures are far more common in the lower limb (~95%) than the upper limb . High-risk sites of stress fractures are locations at greatest risk of a progression to complete fracture, displacement or non-union. These sites are under tensile stresses and have poor vascularity. These include:
- superolateral femoral neck
- anterior tibial cortex
- 5 metatarsal base
- great toe sesamoids (hallux sesamoids)
- talar neck
- posterior cortex of tarsal navicular
- 2to 4metatarsal necks - e,g. March fracture
- medial malleolus
- femoral head
- patella
- pars interarticularis of the lumbar spine
Low-risk sites of a stress fracture are at low risk of complications and are under compressive stresses. They include:
- calcaneus
- pubic rami
- sacrum
- ribs
- proximal humerus/humeral shaft
- posterior medial tibial shaft
- lateral malleolus
- 2 to 4metatarsal shafts
Radiographic features
Plain radiographs have poor sensitivity (15-35%) in early-stage injuries, which increases in late-stage injuries (30-70%), due to possible callus formation.
MRI is the most sensitive modality for diagnosis of a stress fracture and is an important tool to distinguish high and low-risk fractures to help clinicians for management plans and a sensitivity reported to reach close to 100% .
Plain radiograph
Plain radiographs have poor sensitivity in detecting stress fractures, as positive findings may take months to appear. During the first few weeks after the onset of symptoms, x-rays of the affected area may look normal.
Positive findings can include:
- grey cortex sign: subtle loss of cortical density in early-stage stress injury
- increasing sclerosis or cortical thickening along the fracture site
- periosteal reaction/elevation
- may take up to 2 weeks to be detectable
- fracture line
Nuclear medicine
Bone scans can show evidence of stress fracture within a few days upon the onset of symptoms. As a modality, it is considered less sensitive than MRI .
Stress fractures on bone scintigraphy appear as foci of increased radioisotope activity ('hot spot') due to increased bone turnover at the site of new bone formation. However, as with all bone scintigraphy, this is non-specific; the increased uptake can also be due to osteomyelitis, bone tumors or avascular necrosis.
CT
The findings are similar to plain radiography, including sclerosis, new bone formation, periosteal reaction, and fracture lines in long bones.
CT may be useful in differentiating stress fractures from a bone tumor or osteomyelitis if the plain radiographs are negative and bone scans are positive.
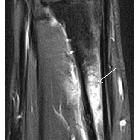
MRI
MRI is the most sensitive modality for detecting stress fracture, and may also be useful for differentiating ligamentous/cartilaginous injury from a bony injury.
Typical MRI appearance of stress fracture includes:
- periosteal or adjacent soft tissue edema
- band-like bone marrow edema
- T1 hypointense fracture line evident in high-grade injury
The use of MRI grading system for bone stress injuries is helpful for predicting recovery time (important especially for athletes).
Treatment and prognosis
Treatment is determined by the site of the stress fracture and suitability for rehabilitation.
Fractures at low-risk sites are managed conservatively with analgesia, ice, reduced weight-bearing and modification of activities until pain resolves.
At high-risk sites or in patients where long-term rehabilitation is detrimental to their livelihood (i.e. athletes or laborers), orthopedic consultation is required.
Risk factors such as diet, vitamin D and calcium should be addressed to prevent recurrence. Other factors such as a gradual return to training and biomechanical evaluation of gait may be required. Bone density evaluation can be considered in patients with recurrent stress fractures, family history of osteoporosis or in stress fractures unexplained by exercise activity.
Differential diagnosis
- osteosarcoma and bone tumors can also present with periosteal reaction
- osteomyelitis has marrow edema and soft tissue swelling
- soft tissue bruise: has edema at the injury site, but little marrow abnormality
Practical points
- in addition to the risk stratification by location, any displacement or proximal femur fractures with a fracture line >50% the width of the femoral neck should also be considered high-risk
Siehe auch:
und weiter:
- fissurale Fraktur
- Osteoid-Osteom
- nicht ossifizierendes Fibrom
- solide Periostreaktion
- Wachstumslinien
- mediales Tibiakantensyndrom
- Morbus van Neck
- fibröser Kortikalisdefekt
- transiente Osteoporose der Hüfte
- differential diagnosis for metatarsal region pain
- Stressfraktur des Schenkelhalses
- Stressfraktur des Femur
- disorganised periosteal reaction
- Verdickung der Kompakta
- Stressfrakturen des Sakrums
- Osteoidosteom der Wirbelsäule
- Stressfraktur Kalkaneus
- metatarsalgia
- pubic ramus stress fracture
- Stressfraktur der Pedikel der LWS
- co-incidence of spontaneous osteonecrosis and stress fracture
- Knochenmarködem-Syndrom (KMÖS)
- Stressfrakturen bei Bisphosphonattherapie
- Stressfraktur der Tibia
- Bisphosphonattherapie assoziierte Femurfrakturen
- FCD
- navicular stress fracture
- longitudinal stress fracture of the tibia
- Stressfraktur proximale Tibia
- proximal tibia stress fracture
- Stressfraktur des Radius
- subtrochanteric stress fracture
- stress fractures in the foot and ankle
- stress fracture of fibula
- Stressfraktur Tibia
- Überlastungsverletzungen bei Kindern
- longitudinal stress fracture
- cortical lesions - bone (mnemonic)
- multiple Stressfrakturen
- proximale Stressfrakturen Os metatarsale 5


 Assoziationen und Differentialdiagnosen zu Stressfraktur:
Assoziationen und Differentialdiagnosen zu Stressfraktur:
