Striatocapsular infarct
Striatocapsular infarcts, also known as basal ganglionic capsular infarcts are infarcts involving the caudate nucleus, putamen, and anterior limb of the internal capsule without any involvement of the cortex, caused by either a complete or partial proximal middle cerebral artery occlusion.
Terminology
Striatocapsular infarcts should be distinguished from lenticulostriate infarcts although the terminology is used inconsistently in the literature, and as such the term large lenticulostriate infarct that is sometimes used should probably be avoided.
A pragmatic approach is to reserve lenticulostriate infarction for lacunar strokes that result from occlusion of a single lenticulostriate perforator. Striatocapsular infracts, in contrast, represent larger infarcts due to occlusion of multiple perforators .
Epidemiology
Historically striatocapsular infarcts were uncommon, but also likely under-recognized, with one landmark series reporting 11 cases out of a stroke registry containing 1,600 patients . More recently, however, they are seen more frequently in patients who have had early treatment of M1 thromboembolic occlusion either by intravenous thrombolysis or endovascular clot retrieval that successfully prevents cortical infarction but does not reperfuse occluded perforators.
Risk factors
Risk factors are thought to be more akin with those of thromboembolic cortical ischemic stroke rather than those of lacunar infarction, with hypertension, smoking, hypercholesterolemia, carotid stenosis, and atrial fibrillation being important risk factors .
Clinical presentation
Although there is a variable clinical presentation, classically patients with striatocapsular infarcts, in the acute phase, exhibit both cortical (e.g. aphasia, sensory neglect or extinction, apraxia) and subcortical (e.g. upper limb hemiparesis, dysarthria) neurological signs, despite the cortex not being directly involved in the infarction . The underlying mechanisms for these cortical signs being present in this subcortical striatocapsular infarction are unfortunately not well understood, but are thought to be due to decreased, but not absent, cortical blood flow, as discussed below .
Pathology
Striatocapsular infarcts are defined as infarcts involving the caudate nucleus, putamen, and anterior limb of the internal capsule that are at least 30 mm in length and 10 mm in width, without the involvement of the overlying cerebral cortex . Although they occur in a similar area to lacunar infarcts and have previously been described as ‘giant lacunes’ or ‘super lacunes’ , they are not only larger than Miller Fisher’s lacune definition but also have different pathogenesis and clinical phenotype .
These infarcts are caused by one of three mechanisms, most often thromboembolic in etiology :
- complete proximal MCA occlusion, or
- partial occlusion of the MCA origin that also blocks lateral lenticulostriate artery origins
- recanalization of M1 occlusion with thrombolysis or endovascular clot retrieval
However, unlike cortical infarcts that may also be due to MCA occlusion, the overlying cortex is not involved in striatocapsular infarcts . This is likely due to either collateral circulation via transcortical and transdural anastomoses, partial MCA occlusion still allowing the MCA to be patent enough to supply blood to the cortex or early recanalization .
Radiographic features
CT/MRI
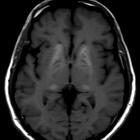
Prominent features that are seen on cross-sectional imaging include:
- infarction of the caudate nucleus, putamen, and anterior limb of the internal capsule
- a characteristic ‘comma’ (or 'lentiform' or 'triangular') shape that is initially hypodense on CT or has increased diffusion signal on DWI (see ischemic stroke for radiographical temporal progression of such lesions)
- no evidence of acute cortical ischemia , although there may be cortical hypoperfusion evident on perfusion studies
- at least 30 mm in length and 10 mm in width in size , although it is not certain how widely accepted these specific measurements are
In addition to initial CT or MRI, it may be useful to perform CT angiography and carotid Doppler ultrasound, as well as other components of the stroke etiology work-up that would be normally performed for a cortical ischemic stroke of likely thromboembolic origin .
History and etymology
The term was coined by Peter Bladin and Samuel Berkovic, Australian neurologists, in their 1984 seminal paper .
Differential diagnosis
- lacunar infarct
- enlarged Virchow-Robin spaces
- cortical ischemic stroke (clinical differential)
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Basal ganglionic capsular infarction:
Assoziationen und Differentialdiagnosen zu Basal ganglionic capsular infarction: