thrombosiertes Aneurysma der Arteria poplitea


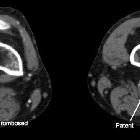





thrombosiertes Aneurysma der Arteria poplitea
Aneurysma der Arteria poplitea Radiopaedia • CC-by-nc-sa 3.0 • de
Popliteal artery aneurysms are the most common peripheral arterial aneurysm and the second most common aneurysm after abdominal aortic aneurysms.
Epidemiology
Overall, popliteal artery aneurysms are uncommon. They occur almost exclusively in males (up to 97%) for unknown reasons . There is an increased incidence with age.
Associations
- strong association with abdominal aortic aneurysms (AAA); ~ 40% of patients with a popliteal artery aneurysm have a AAA, though only 10-15% of patients with AAA have popliteal artery aneurysms
- although rare, connective tissue diseases (e.g. Ehlers-Danlos) are associated with multiple arterial aneurysms at an early age
Clinical presentation
- asymptomatic incidental finding
- pulsatile mass
- may present with complications (see below)
Pathology
Popliteal artery aneurysm are bilateral in 50 to 70% of cases. Their location at the knee point, an area of repeated flexion, may be contributory . They can either be true or false aneurysms:
- true aneurysms of the popliteal artery (commonest) are usually degenerative
- false aneurysms result from trauma, surgery/intervention, or infection
Radiographic features
Ultrasound
- often the initial imaging modality of choice
CT
- CT angiography (CTA) is useful for assessment of vessels distal to the aneurysm
MRI
MR angiography has poorer spatial resolution than CTA and DSA although newer techniques (e.g. contrast-enhanced equilibrium phase imaging) are showing promise
Angiography (DSA)
Angiography can directly show mural calcification and aneurysmal dilatation. Although angiography remains the "gold standard" according to vascular surgery literature, aneurysmal dilatation may be masked by thrombus formation within the aneurysmal sac in ~25% of cases . Instead, it appears as an acute bend in the course of the popliteal artery at the level of the knee joint - this secondary sign is called "dog leg" sign.
Treatment and prognosis
Symptomatic aneurysms are treated. Asymptomatic aneurysms >2 cm diameter also considered for elective treatment:
- endovascular insertion of covered stent: flexible soft device (such as Viabahn stent graft) has better outcome due to movement at the knee crease; 5 year patency rate for Viabahn stent graft is 70%; disadvantages include kinking or fracture of stent due to excessive movement
- open surgical repair (usually aneurysmorrhaphy and bypass surgery): vein graft typically used; 5 year patency rate of vein graft is also 70%
Complications
- distal thromboembolism (commonest: occurs in 18-31% of untreated cases)
- rupture (rare)
- pressure effects if large enough
Differential diagnosis
The differential (mainly clinical due to transmitted pulsations of the popliteal artery) include:
- popliteal cyst (Baker's cyst)
- cystic adventitial disease of the popliteal artery
- other cystic masses in the popliteal masses e.g. synovial sarcoma
Siehe auch:


 Assoziationen und Differentialdiagnosen zu thrombosiertes Aneurysma der Arteria poplitea:
Assoziationen und Differentialdiagnosen zu thrombosiertes Aneurysma der Arteria poplitea:
