synovial sarcoma


























Synovial sarcomas are relatively common intermediate-to-high grade malignant soft tissue tumors, often with an initial indolent course, affecting young patients, and most commonly involving the soft tissue surrounding the knees.
Epidemiology
Synovial sarcomas typically present in adolescents and young adults (15-40 years of age). There may be a mild male predilection (M:F = 1.2:1). They account for 2.5-10% of all soft tissue sarcoma .
Clinical presentation
The presentation is most often with a slowly-enlarging soft tissue mass which may have been noted for some years and gives a false impression of a benign process .
Pathology
Synovial sarcoma derives its name from the fact that microscopically it resembles normal synovium. However, it stains for epithelial markers (e.g. epithelial membrane antigen and cytokeratin), which synovium does not. Additionally, it has been found in many locations that do not normally have synovium.
The most common location for these tumors is within the soft tissues adjacent to large joints, e.g. knee and popliteal fossa. While these tumors arise near joints, it is rare for them to arise from the joint itself and despite their name, they do not arise from synovial structures, e.g. joints, tendon sheaths and bursae.
Macroscopic appearance
Macroscopically they have non-specific appearances. They are well or poorly-defined heterogeneous masses with common areas of hemorrhage and necrosis.
Histology
They are divided histologically into four subtypes:
- biphasic: 20-30%
- monophasic fibrous: 50-60%
- monophasic epithelial: very rare
- poorly differentiated: 15-25%
Genetics
Cytogenetic aberration of the t(X;18) translocation is highly specific, seen in over 90% of cases .
Associations
Synovial sarcoma is one of the (less common) causes of cannonball metastases to the lung.
Location
- extremities: 80-95%
- lower limb: 60-70%
- upper limb: 15-25%
- from soft tissues: 90-95%
- from joint: 5-10%
- head and neck: 5%
- hypopharynx or parapharyngeal space
- conjunctiva
- CNS
- chest wall: rare
- viscera: rare
- lung , kidney, prostate, esophagus, heart, pericardium, pleura
Radiographic features
A soft tissue mass near but not in a joint in a young patient (15-40 years old), particularly if dystrophic calcification is present, are very suggestive.
Plain radiograph
Radiographs may be normal unless the mass is large or contains dystrophic calcifications, which are found in up to 30% of cases . These calcifications are non-specific within the periphery of the lesion and not usually osteoid or chondroid in appearance.
Occasionally, smooth pressure erosions may be visible on the underlying bone, which should not be mistaken for a sign of a benign process.
Alternatively, direct bony invasion is seen in ~30% (range 11-50%) of cases, with aggressive bone features (permeative, geographic, or moth-eaten appearances) .
Ultrasound
Non-specific findings, with a heterogeneous predominantly hypoechoic mass. Intra-lesion flow is usually associated with more aggressive lesions.
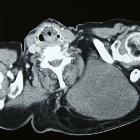
CT
CT is non-specific, similar to ultrasound. It appears as a soft tissue mass of heterogeneous density and enhancement. CT is, of course, more sensitive to calcifications than either radiographs or MRI.
MRI
MRI is the modality of choice to stage the tumor locally, although again imaging findings are not pathognomonic. The mass is usually large and variably well-defined (smaller lesions tend to be better circumscribed).
- T1
- iso- (slightly hyper-) intense to muscle
- heterogeneous
- T2
- mostly hyperintense
- the markedly heterogeneous appearance of synovial cell sarcomas on fluid-sensitive sequences results in so-called "triple sign" which is due to areas of necrosis and cystic degeneration with very high signal, relatively high signal soft tissue components and areas of low signal intensity due to dystrophic calcifications and fibrotic bands
- due to the high tendency of lesions to bleed, there might be areas of fluid-fluid levels known as "bowl of grapes" are seen in up to 10-25% of cases
- T1 C + (Gd)
- enhancement is usually prominent and can be diffuse (40%) heterogeneous (40%) or peripheral (20%)
Nuclear medicine
On bone scan, synovial sarcomas typically have heterogeneously increased dynamic and blood pool uptake, with some increase in delayed images, but usually less intense.
Angiography (DSA)
This imaging test is not usually performed. These tumors are usually hypovascular .
Treatment and prognosis
Treatment involves a combination of surgery and usually adjuvant radiotherapy +/- chemotherapy. Radiotherapy is particularly useful in treating tumors where an adequate clear margin cannot be achieved, and ideally, radiotherapy is administered pre-operatively.
Good prognostic variables include:
- small size
- located in the extremity
- younger age <20 years of age
- solid homogeneous mass
- presence of calcification
- biphasic histology (controversial)
Poor prognostic variables include:
- large size (>5 cm): the most important factor
- located in the trunk or head and neck
- older patients
- cystic/hemorrhagic components
- marked heterogeneity
- histology
- poorly differentiated histology
- rhabdoid cells
- extensive tumor necrosis
- high nuclear grade
- p53 mutations
- high mitotic rate (>10 mitoses per 10 high-power field)
Overall 5-year survival is between 36-76%. Both local recurrence (30-50%) and distant metastases are frequent (40-70%), most commonly to the lungs (~80%), bones (~15%), regional lymph nodes (~10%), followed by chest wall / abdomen (~7.5%) .
Differential diagnosis
General imaging differential considerations include:
- pleomorphic undifferentiated sarcoma
- other sarcomas
- metastatic carcinoma
Siehe auch:
- Osteosarkom
- Liposarkom
- Pleomorphes Undifferenziertes Sarkom
- Weichteilsarkom
- Synovialsarkom der Niere
- Synovialsarkom der Pleura
- Synovialsarkom des Pharynx
- thorakales Synovialsarkom
- Verteilung Synovialsarkom
- Klarzellsarkom der Weichteile
- retroperitoneal synovial sarcoma
- Synovialsarkom Oberschenkel
und weiter:
- Myositis ossificans
- Weichteilverkalkungen
- tumoröse Kalzinose
- radiologisches muskuloskelettales Curriculum
- Knochentumoren
- oberflächliche Weichteilläsionen der Extremitäten
- WHO Klassifikation der Weichteiltumoren
- differential diagnosis of calcified pulmonary densities
- skeletal mass with fluid-fluid levels
- Weichteiltumoren der Extremitäten
- differential diagnosis for metatarsal region pain
- extraskeletal musculoskeletal tumors by compartment
- extraskelettales Chondrosarkom
- Sarkom
- extra skeletal musculoskeletal lesions by compartment
- localised mediastinal malignant mesothelioma
- Flüssigkeit-Flüssigkeitsspiegel
- spindle cell tumours
- Synovialsarkom mit Verkalkungen
- synovial sarcoma of the foot
- solitary mediastinal malignant mesothelioma
- Epitheloidsarkom
- hyperdense pulmonale Raumforderungen
- Lungenmetastasen bei Synovialsarkom
- Synovialsarkom der Prostata
- synovial sarcoma of the acromioclavicular joint
- distribution of synovial sarcoma


 Assoziationen und Differentialdiagnosen zu Synovialsarkom:
Assoziationen und Differentialdiagnosen zu Synovialsarkom: