chondrosarcoma




































Chondrosarcomas are malignant cartilaginous tumors that account for ~25% of all primary malignant bone tumors. They are most commonly found in older patients within the long bones and can arise de novo or secondary from an existing benign cartilaginous neoplasm. On imaging, these tumors have ring-and-arc chondroid matrix mineralization with aggressive features such as lytic pattern, deep endosteal scalloping and soft-tissue extension.
Epidemiology
The typical presentation is in the 4 and 5 decades and there is a slight male predominance of 1.5-2:1.
Clinical presentation
Patients usually present with pain, pathological fracture, a palpable lump or local mass effect. Hyperglycemia can occur as a paraneoplastic syndrome.
Pathology
The histology of chondrosarcomas can differ according to their subtype (see below). In general, these tumors are multilobulated (due to hyaline cartilage nodules) with central high water content and peripheral endochondral ossification. This accounts not only for the high T2 MRI signal (see below) but also for rings and arcs calcification or popcorn calcification.
Grading
Chondrosarcomas are divided into three (sometimes four) grades based primarily on cellularity (see: chondrosarcoma grading).
Subtypes
Chondrosarcomas are either primary, arising de novo, or secondary and arise from a pre-existent cartilaginous mass (see: secondary chondrosarcoma).
Primary
- conventional intramedullary chondrosarcoma (or central chondrosarcoma): low, intermediate or high grade (see: chondrosarcoma grading)
- juxtacortical chondrosarcoma: low, intermediate or high grade
- clear cell chondrosarcoma
- myxoid chondrosarcoma: usually intermediate grade
- mesenchymal chondrosarcoma: usually high grade
- extraskeletal chondrosarcoma
- dedifferentiated chondrosarcoma
Secondary
Arising from pre-existing cartilaginous lesions:
- osteochondroma
- solitary osteochondroma
- hereditary multiple exostoses
- enchondroma
- solitary enchondroma
- Ollier disease
- Maffucci syndrome
Distribution
- long bones: 45% (the reason is that the cartilage is more abundant in the long, tubular bones)
- pelvis: 25% especially around the triradiate cartilage
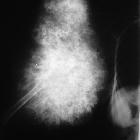
- ribs: 8%
- patients often younger than at other sites
- anterior ribs/costochondral junction
- spine: 7%
- greater male predominance 2-4:1
- thoracic most common
- location
- posterior elements and vertebral body 45%
- posterior elements only 40%
- vertebral body only 15%
- scapula: 5%
- sternum: 2%
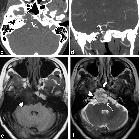
- head and neck (including cervical spine): 6-7%
- craniofacial: 2% (see chondrosarcoma of the skull base)
- hands and feet: rare cf. enchondromas
Radiographic features
Imaging findings vary somewhat with different subtypes but do have some general features. Below are typical imaging appearances which are best demonstrated by conventional chondrosarcomas.
In general chondrosarcomas are large masses at the time of diagnosis, usually >4 cm in diameter and >10 cm in 50% of cases.
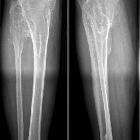
Plain radiograph
- lytic (50%)
- intralesional calcifications: ~70% (rings and arcs calcification or popcorn calcification)
- endosteal scalloping: affecting more than two-thirds of the cortical thickness (c.f. less than two-thirds in enchondromas)
- moth-eaten appearance or permeative appearance in higher grade tumors (see chondrosarcoma grading), e.g. myxoid, dedifferentiated and mesenchymal chondrosarcomas
- cortical remodeling, thickening and periosteal reaction are also useful in distinguishing between an enchondroma and low-grade chondrosarcoma (see enchondroma vs. low-grade chondrosarcoma)
CT
The features seen on CT are the same as on plain film, but are simply better seen:
- 94% of cases demonstrate matrix calcification, c.f. 60-78% on plain film
- endosteal scalloping
- cortical breach, seen in ~90% of long bone chondrosarcoma, c.f. only ~10% of enchondromas
- soft tissue mass: tumor cellularity, and therefore density, increases with increased grade of the tumor
- heterogenous contrast enhancement
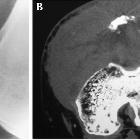
MRI
- T1: low to intermediate signal
- iso- to slightly hyperintense cf. muscle
- iso- to slightly hypointense cf. grey matter (see chondrosarcoma of the base of skull)
- T2: very high intensity in non-mineralized/calcified portions
- gradient echo/SWI: blooming of mineralized/calcified portions
- T1 C+ (Gd)
- most demonstrate heterogeneous moderate to intense contrast enhancement.
- enhancement can be septal and peripheral rim-like corresponding to fibrovascular septation between lobules of hyaline cartilage
Nuclear medicine
Typically chondrosarcomas demonstrate increased uptake on bone scan, seen in over 80% of cases, and usually the uptake is quite intense. This is useful in helping to distinguish low-grade chondrosarcoma from an enchondroma as the latter has increased uptake in ~20% of cases, and usually to a lesser degree (see: enchondroma vs low grade chondrosarcoma).
Treatment and prognosis
Prognosis varies with both grade and location. In general:
- grade
- grade 1: 90% 5-year survival
- grade 3: 29% 5-year survival
- location
- long bones have a better prognosis than axial skeleton
Siehe auch:
- endosteal scalloping
- Periostreaktion
- Enchondrom
- kartilaginäre Exostose
- Ollier-Syndrom
- Multiple kartilaginäre Exostosen
- popkornartige Verkalkungen
- Maffucci-Syndrom
- juxtakortikales Chondrosarkom
- Unterscheidung Enchondrom Chondrosarkom
- mesenchymal chondrosarcoma
- Skelettszintigraphie
- ring- und bogenförmige Verkalkungen
- Chondrosarkom der Schädelbasis
- extraskelettales Chondrosarkom
- myxoides Chondrosarkom
- klarzelliges Chondrosarkom
- Chondrosarkom des Femurs
- permeative process
- Chondrosarkom der Kieferhöhle
- konventionelles Chondrosarkom
- entdifferenziertes Chondrosarkom
- Chondrosarkom Grading
- mesenchymal chondrosarcomas
und weiter:
- Codman-Dreieck
- Cholesterolgranulom der Felsenbeinspitze
- Meningeom
- Chordom
- Tumor Kleinhirnbrückenwinkel
- Riesenzelltumor
- neuroradiologisches Curriculum
- Chondrom
- Chondrosarkom der Rippen
- diabetisches Fußsyndrom
- radiologisches muskuloskelettales Curriculum
- Knochentumoren
- Karzinom des Nasopharynx
- Gradenigo-Syndrom
- Riesenzelltumor des Knochens
- differential diagnosis of calcified pulmonary densities
- Cavum trigeminale
- arrested pneumatization of skull base
- Ostitis fibrosa cystica
- Osteoklastom
- Raumforderungen im oder am Sinus cavernosus
- differential diagnosis for calcified masses in the mandible
- Sarkom
- Chondrosarkom des Clivus
- cementifying fibroma
- disorganised periosteal reaction
- Läsionen der Mandibula
- chondroide Tumoren
- Chondrosarkom der Pleura
- Chondrosarkom des proximalen Femurs
- Knochenläsionen der Metaphyse
- secondary chondrosarcoma
- Pyramidenspitzen-Osteomyelitis
- low-grade chondrosarcoma
- Chondrosarkom der Skapula
- Chondrosarkom des Os sacrum
- arrested pneumatisation of the skull base
- Chondrosarkom des Sternums
- Chondrosarkom des Larynx
- klarzelliges Chondrosarkom des Hüftkopfes
- hyperdense pulmonale Raumforderungen
- sarcomatous degeneration bone exostosis
- Chondrosarkom Wirbelsäule
- Chondrosarkom Metastasen
- Chondrosarkom des Zungenbeins


 Assoziationen und Differentialdiagnosen zu Chondrosarkom:
Assoziationen und Differentialdiagnosen zu Chondrosarkom: