CSF hygromas














Subdural hygromas (alternative plural: hygromata ) refer to the accumulation of fluid in the subdural space. In many cases, it is considered an epiphenomenon of head injury when it is called a traumatic subdural hygroma.
Epidemiology
Subdural hygromas are encountered in all age-groups but are overall most common in the elderly . The demographics will depend on the underlying cause which includes:
- idiopathic: in pediatric patients
- trauma
- post surgical, e.g. hematoma evacuation, ventricular drainage
- spontaneous intracranial hypotension
Clinical presentation
The vast majority of patients are asymptomatic. However, some symptoms uncommonly reported include :
- headaches
- changes in mental status
- nausea and vomiting
- focal neurological deficits
- seizures
Pathology
The pathogenesis of subdural hygromas is not entirely understood. The most commonly encountered explanation is a tear in the arachnoid layer forming a ball-valve opening allowing CSF one way passage into the subdural space. Although this explanation has the benefit of simplicity, it does not necessarily represent a true description of the underlying mechanisms. It has been proposed that subdural hygromas, at least sometimes, represent prominent subdural effusions in which there is a separation of the dural border cell layer with an accumulation of fluid . There is undoubtedly a relationship between subdural hygromas and acute on chronic and chronic subdural hematomas .
Radiographic features
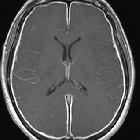
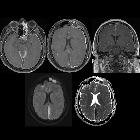
Subdural hygromas generally occur along the supratentorial cerebral convexities; occurrence in the posterior fossa is rare .
CT/MRI
A subdural hygroma radiographically appears as a crescentic near-CSF density/signal accumulation in the subdural space that does not extend into the sulci and rarely exerts significant mass-effect . Vessels rarely cross through the lesion in contrast-enhanced studies (see cortical vein sign) . Importantly these collections do not entirely follow CSF on FLAIR, often appearing hyperintense.
Treatment and prognosis
The vast majority of patients with subdural hygroma are asymptomatic without radiographic evidence of mass-effect, and thus neurosurgical intervention is rarely required . In cases where mass-effect is radiographically demonstrated, it may be neurosurgically evacuated .
Differential diagnosis
Imaging differential considerations include:
- chronic subdural hematoma
- the relationship between chronic subdural hematomas and subdural hygromas is complex and incompletely understood
- it is almost certain that a significant number of collections diagnosed as chronic subdural hematomas represent chronic subdural hygromas
- MRI may be required to differentiate as they can have an identical appearance on CT but it should be noted that subdural hygromas often do not completely follow CSF on FLAIR
- cerebral atrophy
- involutional change with enlargement of the subarachnoid space
- a positive cortical vein sign may indicate this instead
- arachnoid cyst
- rounded and circumscribed with localized mass effect
- completely follows CSF on all sequences
- benign enlargement of the subarachnoid spaces in infancy
- a positive cortical vein sign may indicate this instead
Siehe auch:
- Arachnoidalzyste
- Hirnabszess
- subdurales Hämatom
- Empyem
- Meningitis
- subdurales Empyem
- Mastoiditis
- Hygrom
- intrakranielle Infektionen
- chronisches Subduralhämatom
- venous infarction
- epidural empyemas
und weiter:


 Assoziationen und Differentialdiagnosen zu subdurales Hygrom:
Assoziationen und Differentialdiagnosen zu subdurales Hygrom: