UIP
































Usual interstitial pneumonia (UIP) is a histopathologic and radiologic pattern of interstitial lung disease, which is the hallmark pattern for idiopathic pulmonary fibrosis (IPF).
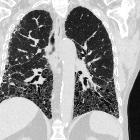
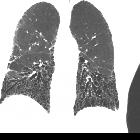
On imaging, usual interstitial pneumonia usually presents with a lung volume loss and a craniocaudal gradient of peripheral septal thickening, bronchiectasis, and honeycombing.
This article will focus solely on the usual interstitial pneumonia pattern as a radiological or histopathological descriptor, for further discussion in the clinical aspects, please refer to the parental article on the specific underlying clinical diagnosis (e.g. idiopathic pulmonary fibrosis).
Terminology
In the past, the term usual interstitial pneumonia was used synonymously with idiopathic pulmonary fibrosis. However more recently the term idiopathic pulmonary fibrosis has been applied solely to the clinical syndrome associated with the morphologic pattern of UIP, with the specific exclusion of entities such as non-specific interstitial pneumonia (NSIP) and desquamative interstitial pneumonia (DIP) .
Pathology
The histological diagnosis of UIP is based on temporal and spatial heterogeneity, which is the identification of fibrotic lesions at different stages (fibroblastic infiltrates, mature fibrosis, and honeycombing) within the same biopsy specimen and architectural distortion. Honeycombing, particularly if it involves more than 5% of the lung volume, is an almost 100% specific finding. On a typical biopsy, there are areas of normal lung alternating with interstitial fibrosis and honeycombing. The distribution of UIP characteristically is with an apicobasal gradient with basal and peripheral (subpleural) predominance, although it is often patchy.
Inflammation is absent or mild and mostly limited to the areas of honeycombing .
Etiology
UIP pattern of ILD can be seen in idiopathic pulmonary fibrosis or secondary to underlying systemic diseases. These would include:
- connective tissue disorders (CTD associated UIP): falls under the borader spectrum of connective tissue disorder interstitial lung disease (CTD-ILD)
- rheumatoid arthritis: UIP is considered to be the dominant pattern in those with rheumatoid arthritis who have concurrent interstitial lung disease
- systemic sclerosis (scleroderma): either a UIP or NSIP (commoner) pattern
- polymyositis/dermatomyositis: a UIP, NSIP, or COP pattern
- mixed connective tissue disease: either a UIP or NSIP pattern
- asbestos-related interstitial lung disease: asbestosis
- chronic hypersensitivity pneumonitis
- radiation
- medications/drug toxicity: amiodarone lung
- ANCA associated vasculitides
- Hermansky-Pudlak syndrome (very rare)
In practice, the diagnosis is usually made in a multidisciplinary approach involving chest physicians, radiologists and pathologists with expertise in interstitial lung disease (ILD) .
Radiographic features
Plain radiograph
Plain film features are non-specific. While chest radiographs can be even normal in patients with very early disease, in advanced disease, it may show decreased lung volumes and basal fine to coarse reticulation. Usually, due to the more extensive involvement of the lower lobes, the major fissure is shifted inferiorly which is best seen on the lateral chest radiograph.
CT
When describing imaging features, the term UIP pattern is often used, which has specific diagnostic criteria on HRCT . The positive predictive value of CT in the diagnosis of UIP is high and ranges from 70-100% . Similar to the pathology specimen, cross-sectional imaging also reveals heterogeneity, with patchy areas of fibrosis alternating with areas of normal lung .
Typical features include :
- honeycombing: particularly if it involves more than 8% of the lung parenchyma, is highly specific for UIP. In general, UIP can be divided into two groups, those with <5% honeycombing and those with >5% honeycombing. It mainly reflects the stage and severity of the disease. Those with less than 5% honeycombing may pose diagnostic difficulty as differentiation from NSIP on imaging can be impossible; however, these still follow similar prognosis as other UIP patients
- reticular opacities: in the immediate subpleural lung, often associated with honeycombing and traction bronchiectasis, with peripheral and lower lobe predominance, is considered a very good differentiating feature from patients with NSIP and concurrent emphysema
- reticular opacity-to-ground glass opacity ratio: one or greater
- ground-glass opacities: usually less extensive than the reticular pattern and almost never seen in isolation - usually happens in areas of reticulation or honeycombing
- lung architectural distortion: which reflects lung fibrosis and is often prominent
- lobar volume loss (predominantly lower lobes) is seen in cases of more advanced fibrosis
In recent times some authors have suggested certain signs within a UIP pattern more suggestive of it being due to connective tissue disorder interstitial lung disease over IPF
These include
- straight-edge sign: isolation of fibrosis to bases with a sharp demarcation in the craniocaudal plane without substantial extension along the lateral margins of the lungs on coronal images
- anterior upper lobe sign: concentration of fibrosis along the anterior aspect of the upper lobes with relative sparing of the other aspects of the upper lobes but with concomitant lower lobe involvement
- exuberant honeycombing sign: exuberant honeycomb-like cyst formation within the lungs constituting greater than 70% of fibrotic portions of lung
Diagnostic criteria
See articles:
- diagnostic HRCT criteria for UIP pattern - ATS/ERS/JRS/ALAT (2018)
- diagnostic HRCT criteria for UIP pattern - Fleischner society guideline (2018)
Treatment and prognosis
In patients with UIP, areas of ground-glass attenuation tend to increase in extent or progress to fibrosis despite treatment . In those with more active inflammation involving the pulmonary interstitium, there is a faster progression of honeycombing in long-term follow-up . The average rate of progression of honeycombing in patients with idiopathic usual interstitial pneumonia according to one study was 0.4% of lung volume per month .
Differential diagnosis
A key imaging differential on cross-sectional imaging would be:
- non-specific interstitial pneumonia pattern (especially fibrotic non-specific interstitial pneumonia)
- chronic hypersensitivity pneumonitis (HP)
- HP usually involves the mid and upper zones of the lung, and also the presence of centrilobular nodules and areas of air trapping are very useful hints to differentiate it from UIP
- UIP cases are also thought to have honeycombing and peripheral or lower lung zone predominance of disease, and less likely to have micronodules
- amiodarone lung fibrosis: helpful clues are the presence of hyperdense pulmonary nodules or hyperdense liver on a non-contrast CT
- systemic sclerosis: presence of patulous esophagus and correlation with hand radiographs if available can be helpful
- asbestosis: bilateral pleural plaques with or without calcification or peritoneal calcification are helpful in diagnosis
- combined pulmonary fibrosis and emphysema (CPFE): especially if there is added upper lobe-predominant emphysema
Siehe auch:
- Honigwabenmuster
- Milchglasverschattungen
- Traktionsbronchiektasen
- non specific interstitial pneumonia (NSIP)
- Diagnostic HRCT criteria for usual interstitial pneumonia (UIP) pattern - Fleischner society guideline (2018)
- retikuläres Muster
- pulmonary manifestations of scleroderma
- Diagnostic HRCT criteria for usual interstitial pneumonia (UIP) pattern - ATS/ERS/JRS/ALAT (2018)
- chronic hypersensitivity pneumonitis
- combined pulmonary fibrosis and emphysema
- lung architectural distortion
- typical UIP CT pattern
- probable UIP pattern
- Amiodaronlunge
- asbestos related pulmonary fibrosis
- indeterminate for UIP pattern
- fibrotic non-specific interstitial pneumonia
und weiter:
- verdickte interlobuläre Septen
- multiple zystische Lungenherde
- pulmonale und mediastinale Sarcoidose
- reticular and linear pulmonary opacification
- idiopathic interstitial pneumonia (mnemonic)
- pulmonary opacification
- crazy paving-Muster
- Interstitielle Lungenerkrankung
- interstitial pneumonia
- Honigwabenlunge
- pulmonale Manifestationen rheumatoide Arthritis
- Nicht spezifische interstitielle Pneumonie (NSIP)
- What Every Radiologist Should Know about Idiopathic Interstitial Pneumonias
- peripheral lung opacities (mnemonic)
- Desquamative interstitielle Pneumonie (DIP)
- subpleurale Fibrose
- Idiopathische interstitielle Pneumonie
- CT features most consistent with non-IPF diagnosis
- Fibrose UIP


 Assoziationen und Differentialdiagnosen zu gewöhnliche interstitielle Pneumonie (UIP):
Assoziationen und Differentialdiagnosen zu gewöhnliche interstitielle Pneumonie (UIP): 





