diffuse axonal injury (DAI)


























Diffuse axonal injury (DAI), also known as traumatic axonal injury (TAI), is a severe form of traumatic brain injury due to shearing forces. It is a potentially difficult diagnosis to make on imaging alone, especially on CT as the finding can be subtle, however, it has the potential to result in severe neurological impairment.
The diagnosis is best made on MRI where it is characterized by several small regions of susceptibility artifact at the grey-white matter junction, in the corpus callosum, and in more severe cases in the brainstem, surrounded by FLAIR hyperintensity.
Epidemiology
The patients at risk of diffuse axonal injury belong to the same cohort as those who suffer traumatic brain injury and as such young men are very much over-represented.
Clinical presentation
Typically, patients who are shown to have diffuse axonal injury have loss of consciousness at the time of the accident. Post-traumatic coma may last a considerable time and is often attributed to coexistent more visible injury (e.g. cerebral contusions). As such the diagnosis is often not suspected until later when patients fail to recover neurologically as expected.
Pathology
Diffuse axonal injury is the result of shearing forces, typically from rotational acceleration (most often a deceleration). Due to the slightly different specific gravities (relative mass per unit volume) of white and grey matter, shearing due to change in velocity has a predilection for axons at the grey-white matter junction, as the name implies. In the majority of cases, these forces result in damage to the cells and result in edema. Actual complete tearing of the axons is only seen in severe cases. It is also known that some neurons may undergo degeneration in the weeks or months after trauma, it is called secondary axonotmesis.
Associations
Radiographic features
Diffuse axonal injury is characterized by multiple focal lesions with a characteristic distribution: typically located at the grey-white matter junction, in the corpus callosum and in more severe cases in the brainstem (see: grading of diffuse axonal injury).
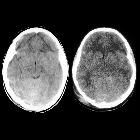
CT
Non-contrast CT of the brain is routine in patients presenting with head injuries. Unfortunately, it is not sensitive to subtle diffuse axonal injury and as such, some patients with relatively normal CT scans may have significant unexplained neurological deficit .
The appearance depends on whether or not the lesions are overtly hemorrhagic. Hemorrhagic lesions will be hyperdense and range in size from a few millimeters to a few centimeters in diameter. Non-hemorrhagic lesions are hypodense. They typically become more evident over the first few days as edema develops around them. They may be associated with significant and disproportionate cerebral swelling.
CT is particularly insensitive to non-hemorrhagic lesions (as defined by CT) only able to detect 19% of such lesions, compared to 92% using T2 weighted imaging . When lesions are hemorrhagic, and especially when they are large, then CT is quite sensitive. As such, it is usually a safe assumption that if a couple of small hemorrhagic lesions are visible on CT, the degree of damage is much greater.
MRI
MRI is the modality of choice for assessing suspected diffuse axonal injury even in patients with entirely normal CT of the brain . MRI, especially SWI or GRE sequences, exquisitely sensitive to paramagnetic blood products may demonstrate small regions of susceptibility artefact at the grey-white matter junction, in the corpus callosum or the brain stem. Some lesions may be entirely non-hemorrhagic (even using high field strength SWI sequences). These will, however, be visible as regions of high FLAIR signal.
Over the first few days, the degree of surrounding edema will typically increase, although by 3-months post-injury FLAIR changes will have largely resolved . In contrast, SWI changes will usually take longer to resolve, although by 12-months post-injury there will have been substantial resolution . This is to be expected as edema is faster to resolve than hemorrhage.
In the months that follow the trauma, there is accelerated brain volume reduction, which can sometimes be detected by visual inspection, but sometimes only by volumetric studies.
Importantly, it should be noted, that even with high field strength modern scanners, the absence of findings does not categorically exclude the presence of axonal injury.
MR spectroscopy
MRS can be of benefit in identifying patients with grade I injury which may be inapparent on other sequences. Features typically demonstrate elevation of choline peak and reduction of NAA .
Treatment and prognosis
Unfortunately little can be done for patients with diffuse axonal injury other than providing supportive care trying to minimize secondary damage caused by cerebral edema, hypoxia, seizures, etc. Management involves the early recognition and treatment of neurosurgical complications such as herniation and hydrocephalus.
Depending on the severity and distribution of injury (see: grading of diffuse axonal injury) patients can vary from minimally affected to be in a persistent vegetative state . The amount of axonal injury in the brainstem is predictive of long-term vegetative state, whereas supratentorial injury can result in focal neurological or neuropsychiatric deficits .
Differential diagnosis
On imaging consider:
- cortical contusions
- the main differential in patients with head injuries
- typically located superficially, involving the cortex (rather than at the grey-white matter junction) and are usually associated with variable amounts of extra-axial blood (subarachnoid and subdural)
- diffuse vascular injuries
- particularly on T2* sequences
Siehe auch:
- Kavernom
- zerebrale Mikroblutungen
- Suszeptibilitätsgewichtete Bildgebung
- zerebrale Kontusionsblutung
- grading of diffuse axonal injury
- cortical contusions
und weiter:
- Cytotoxic lesions of the corpus callosum (CLOCCs)
- Balkenläsionen
- zerebrale Kavernome
- neuroradiologisches Curriculum
- wallerian degeneration
- Tumor im Corpus callosum
- zerebrale Fettembolie
- familial multiple cavernous malformation syndrome
- Duret Blutungen
- diffusionsgewichtete Bildgebung
- Marchiafava-Bignami-Syndrom
- intermediary injury
- boomerang sign
- DAI grading
- Frakturen Os temporale


 Assoziationen und Differentialdiagnosen zu Diffuses axonales Schädelhirntrauma:
Assoziationen und Differentialdiagnosen zu Diffuses axonales Schädelhirntrauma:


